| Authors | Stewart RA, White HD, Kirby AC, Heritier SR, Simes RJ, Nestel PJ, West MJ, Colquhoun DM, Tonkin AM; Long-Term Intervention With Pravastatin in Ischemic Disease (LIPID) Study Investigators. | |
| Title | White blood cell count predicts reduction in coronary heart disease mortality with pravastatin | |
| Full source | Circulation. 2005 Apr 12;111(14):1756-62. Epub 2005 Apr 4 | |
|
|
Per scorrere le diapositive |
|
| Abstract | BACKGROUND:
Elevated serum inflammatory marker levels are associated with a greater
long-term risk of cardiovascular events. Because 3-hydroxy-3-methylglutaryl
coenzyme-A reductase inhibitors (statins) may have an antiinflammatory action,
it has been suggested that patients with elevated inflammatory marker levels
may have a greater reduction in cardiovascular risk with statin treatment.
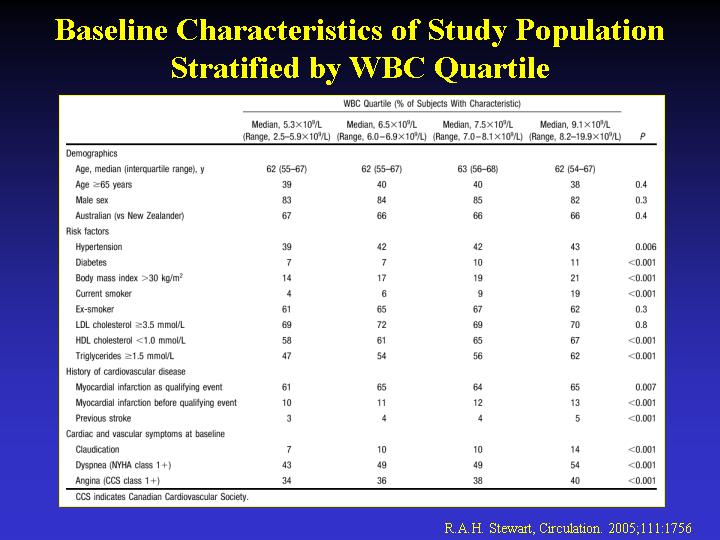
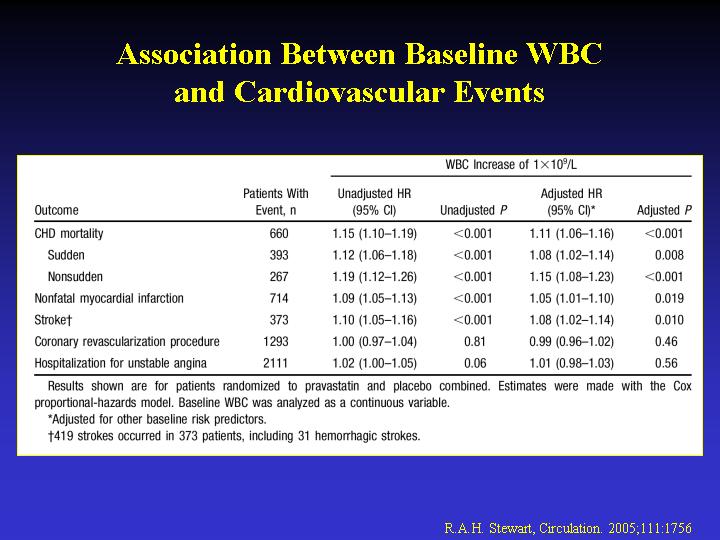
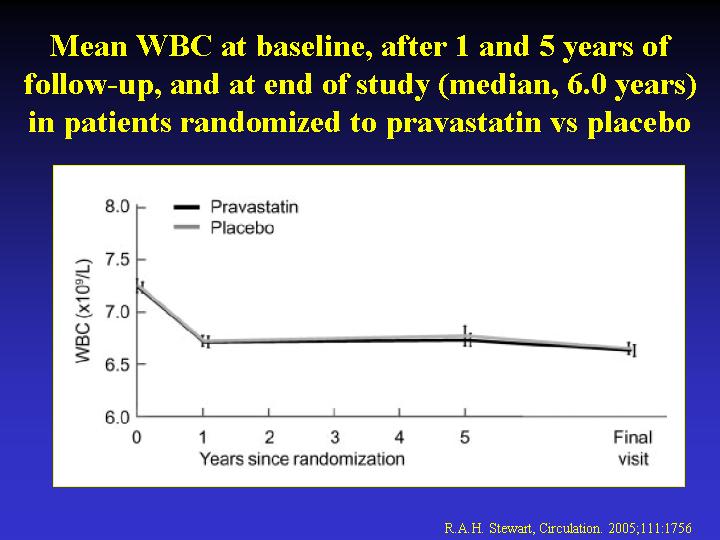
METHODS AND RESULTS: We evaluated the association between the white blood
cell count (WBC) and coronary heart disease mortality during a mean follow-up
of 6.0 years in the Long-Term Intervention With Pravastatin in Ischemic
Disease (LIPID) Study, a clinical trial comparing pravastatin (40 mg/d)
with a placebo in 9014 stable patients with previous myocardial infarction
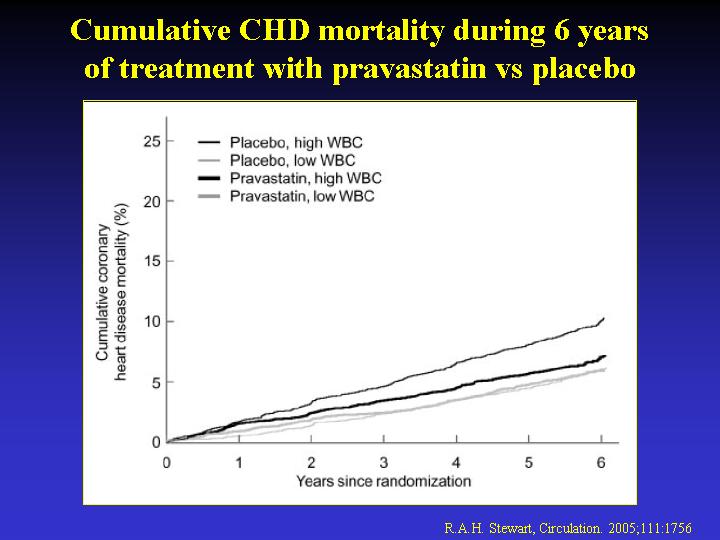
or unstable angina. An increase in baseline WBC was associated with greater
coronary heart disease mortality in patients randomized to placebo (hazard
ratio for 1x10(9)/L increase in WBC, 1.18; 95% CI, 1.12 to 1.25; P<0.001)
but not pravastatin (hazard ratio, 1.02; 95% CI, 0.96 to 1.09; P=0.56; P
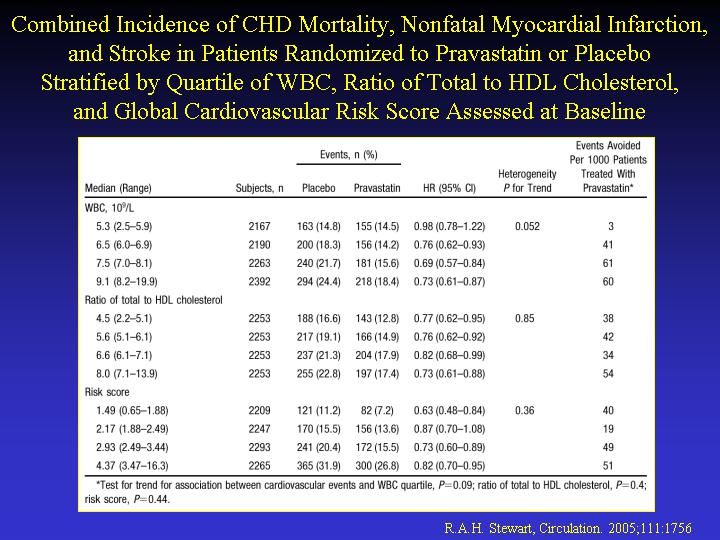
for interaction=0.004). The numbers of coronary heart disease deaths prevented
per 1000 patients treated with pravastatin were 0, 9, 30, and 38 for baseline
WBC quartiles of <5.9, 6.0 to 6.9, 7.0 to 8.1, and >8.2x10(9)/L, respectively.
WBC was a stronger predictor of this treatment benefit than the ratio of
total to high-density lipoprotein cholesterol and a global measure of cardiac
risk. There was also a greater reduction (P=0.052) in the combined incidence
of cardiovascular mortality, nonfatal myocardial infarction, and stroke
with pravastatin as baseline WBC increased (by quartile: 3, 41, 61, and
60 events prevented per 1000 patients treated, respectively). CONCLUSIONS:
These data support the hypothesis that individuals with evidence of inflammation
may obtain a greater benefit from statin therapy. |
|