| Abstract |
BACKGROUND:
High C-reactive protein (CRP) is associated with increased coronary heart
disease risk. Few long-term data in the elderly are available.
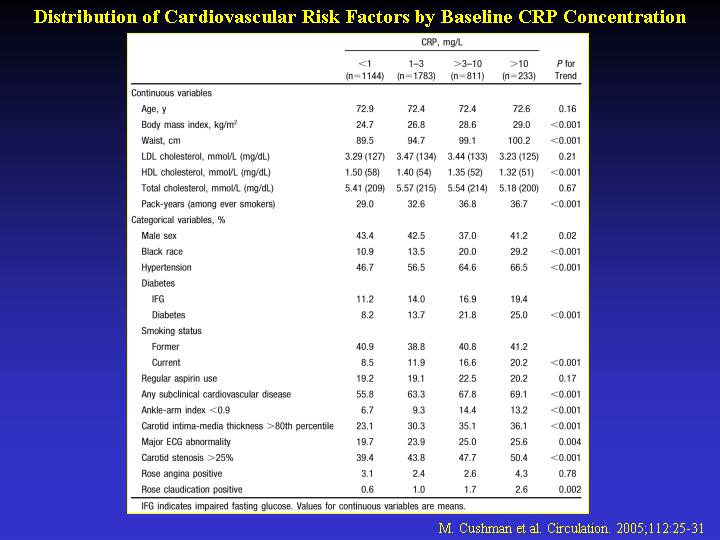
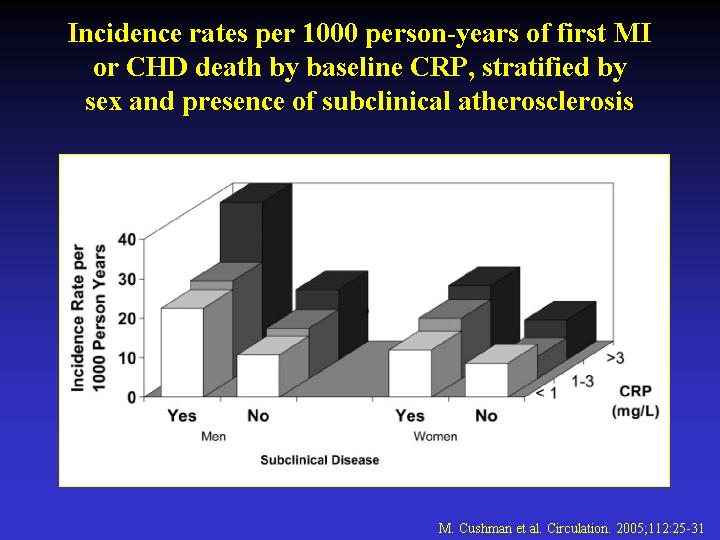
METHODS AND RESULTS: Baseline CRP was measured in 3971 men and women >
or =65 years of age without prior vascular diseases; 26% had elevated
concentrations (>3 mg/L). With 10 years of follow-up, 547 participants
developed coronary heart disease (CHD; defined as myocardial infarction
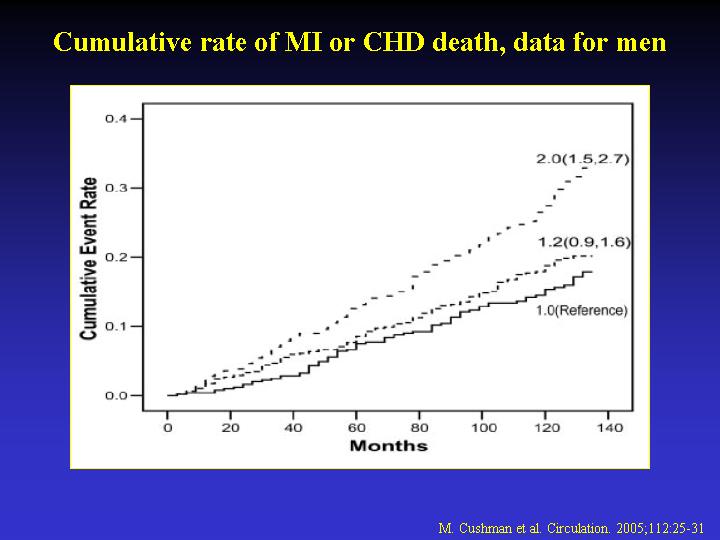
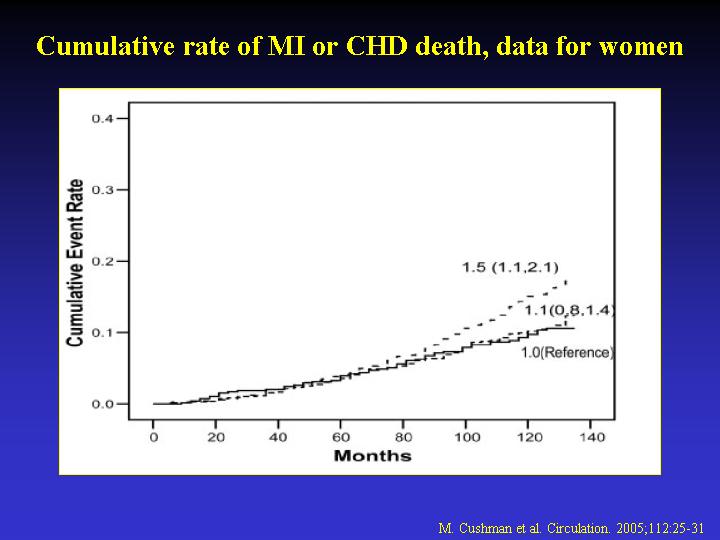
or coronary death). With elevated CRP, the 10-year cumulative CHD incidences
were 33% in men and 17% in women. The age-, ethnicity-, and sex-adjusted
relative risk of CHD for CRP >3 mg/L compared with <1 mg/L was 1.82
(95% CI, 1.46 to 2.28). Adjusting for conventional risk factors reduced
the relative risk to 1.45 (95% CI, 1.14 to 1.86). The population-attributable
risk of CHD for elevated CRP was 11%. Risk relationships did not differ
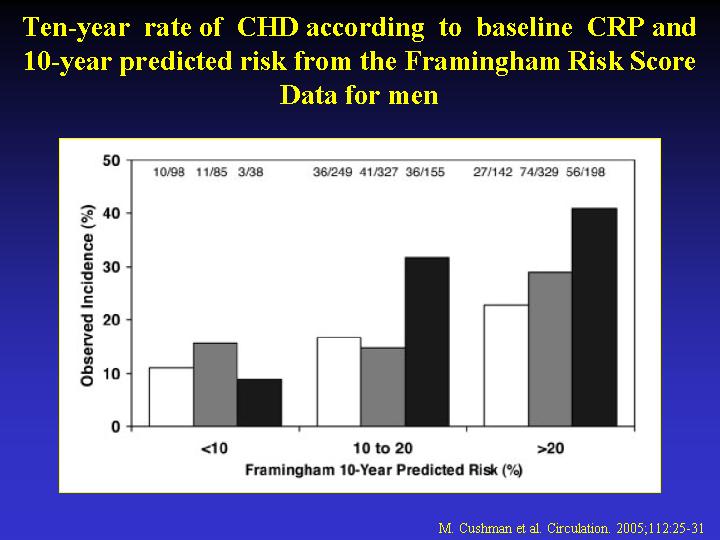
in subgroups defined by baseline risk factors. We assessed whether CRP
improved prediction by the Framingham Risk Score. Among men with a 10-year
Framingham-predicted risk of 10% to 20%, the observed CHD incidence was
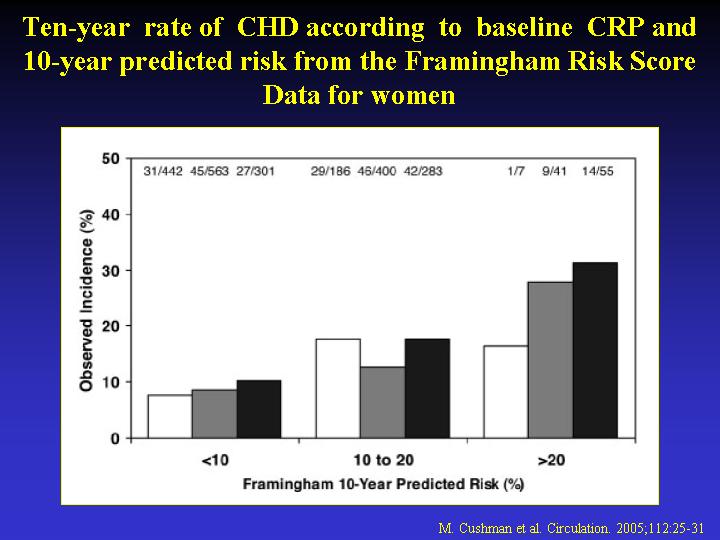
32% for elevated CRP. Among women, CRP discriminated best among those
with a 10-year predicted risk >20%; the incidences were 31% and 10%
for elevated and normal CRP levels, respectively.
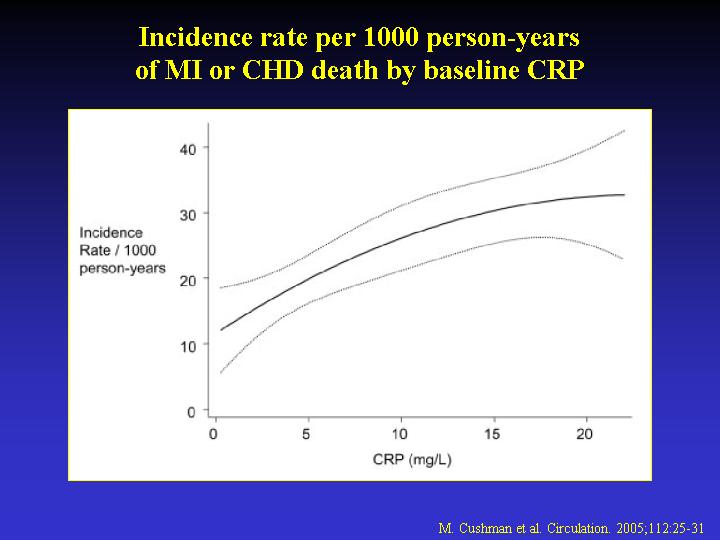
CONCLUSIONS: In older men and women, elevated CRP was associated with
increased 10-year risk of CHD, regardless of the presence or absence of
cardiac risk factors. A single CRP measurement provided information beyond
conventional risk assessment, especially in intermediate-Framingham-risk
men and high-Framingham-risk women.
|