| Abstract |
BACKGROUND:
No therapy has been shown to improve survival in heart failure (HF) with
a normal ejection fraction (EF). There are plausible reasons to hypothesize
that statins may be of benefit in HF with a normal EF.
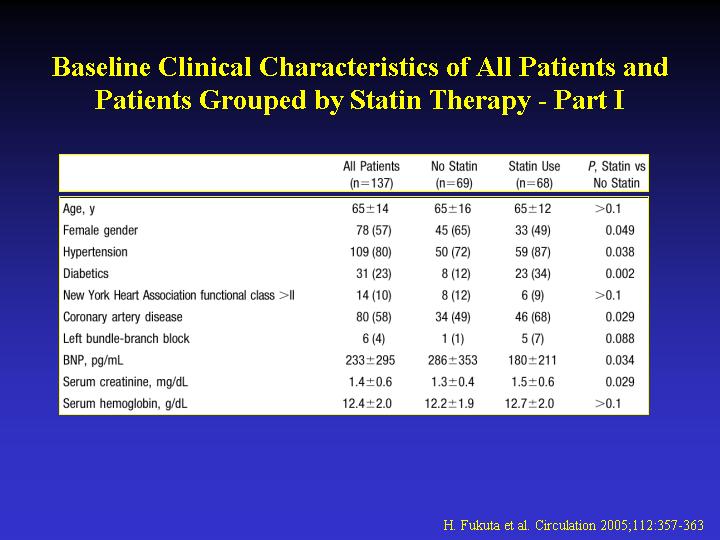
METHODS AND RESULTS: We evaluated 137 patients with HF and an EF >
or =0.50. The effect of treatment received at study entry on survival
was determined. During a follow-up of 21+/-12 months, 20 deaths were observed.
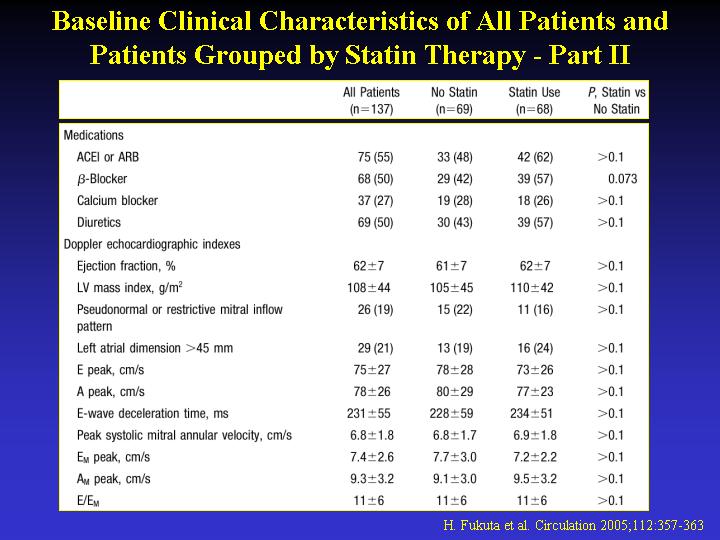
Treatment with an ACE inhibitor or receptor blocker, beta-blocker, or
calcium blocker had no significant effect on survival. In contrast, treatment
with a statin was associated with a substantial improvement in survival
(relative risk of death [95% CI] 0.22 [0.07 to 0.64]; P=0.006). Patients
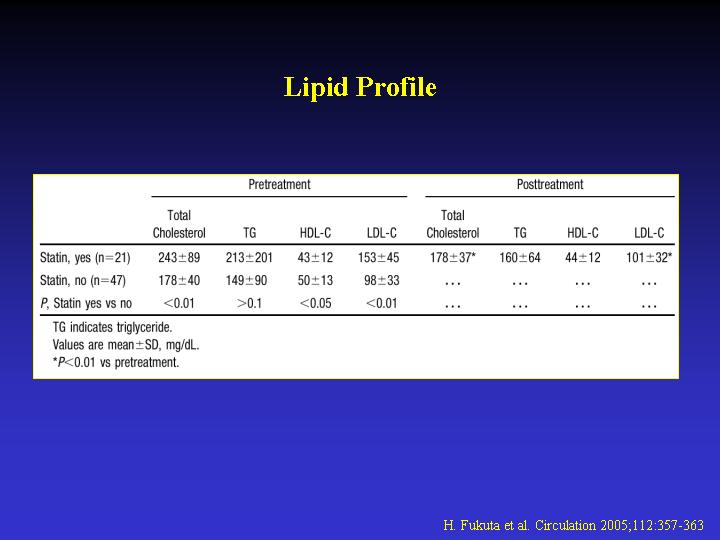
receiving statins had higher baseline LDL cholesterol than those not receiving
statins (153+/-45 versus 98+/-33 mg/dL, P<0.01). After statin therapy,
LDL cholesterol levels fell to a similar level (101+/-32 mg/dL) as in
patients not receiving statins (98+/-33 mg/dL). After adjustment for differences
in baseline clinical variables between groups (hypertension, diabetes,
coronary artery disease, and serum creatinine), statin therapy was associated
with lower mortality (adjusted relative risk of death [95% CI] 0.20 [0.06
to 0.62]; P=0.005). Similarly, after propensity matching, statin therapy
was associated with improved survival (log-rank 6.12; P=0.013) and a trend
toward improved survival without cardiovascular hospitalization (log-rank
3.02; P=0.082).
CONCLUSIONS: Statin therapy may be associated with improved survival in
patients with HF and a normal EF.
|