| Abstract |
BACKGROUND:
Effective early management of patients with transient ischaemic attacks
(TIA) is undermined by an inability to predict who is at highest early
risk of stroke.
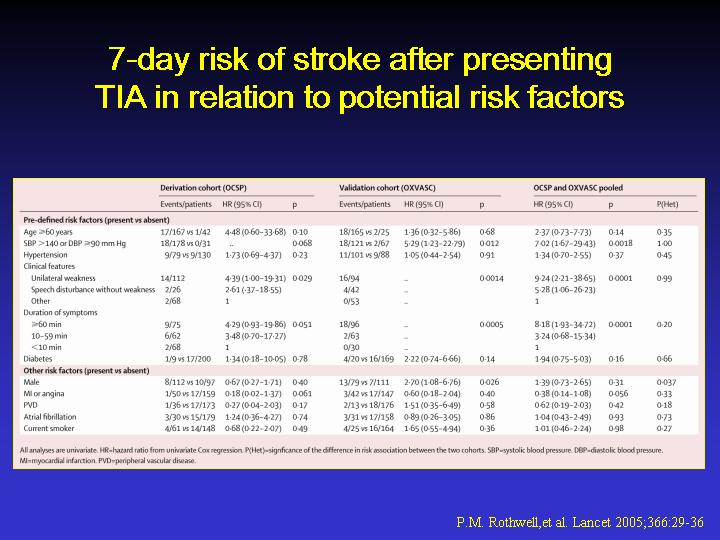
METHODS: We derived a score for 7-day risk of stroke in a population-based
cohort of patients (n=209) with a probable or definite TIA (Oxfordshire
Community Stroke Project; OCSP), and validated the score in a similar
population-based cohort (Oxford Vascular Study; OXVASC, n=190). We assessed
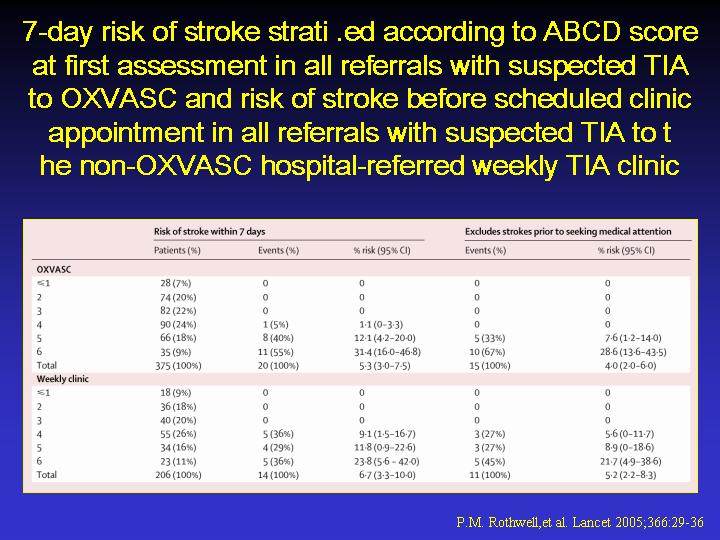
likely clinical usefulness to front-line health services by using the
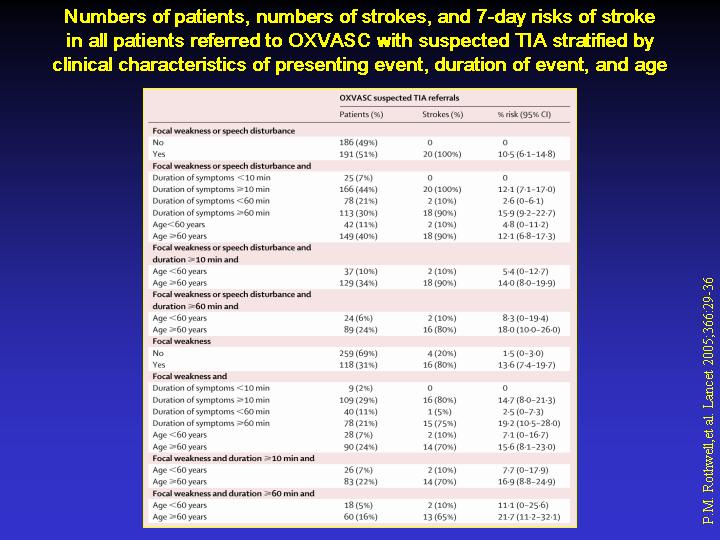
score to stratify all patients with suspected TIA referred to OXVASC (n=378,
outcome: 7-day risk of stroke) and to a hospital-based weekly TIA clinic
(n=210; outcome: risk of stroke before appointment).
RESULTS: A six-point score derived in the OCSP (age [> or =60 years=1],
blood pressure [systolic >140 mm Hg and/or diastolic > or =90 mm
Hg=1], clinical features [unilateral weakness=2, speech disturbance without
weakness=1, other=0], and duration of symptoms in min [> or =60=2,
10-59=1, <10=0]; ABCD) was highly predictive of 7-day risk of stroke
in OXVASC patients with probable or definite TIA (p<0.0001), in the
OXVASC population-based cohort of all referrals with suspected TIA (p<0.0001),
and in the hospital-based weekly TIA clinic-referred cohort (p=0.006).
In the OXVASC suspected TIA cohort, 19 of 20 (95%) strokes occurred in
101 (27%) patients with a score of 5 or greater: 7-day risk was 0.4% (95%
CI 0-1.1) in 274 (73%) patients with a score less than 5, 12.1% (4.2-20.0)
in 66 (18%) with a score of 5, and 31.4% (16.0-46.8) in 35 (9%) with a
score of 6. In the hospital-referred clinic cohort, 14 (7.5%) patients
had a stroke before their scheduled appointment, all with a score of 4
or greater.
CONCLUSIONS: Risk of stroke during the 7 days after TIA seems to be highly
predictable. Although further validations and refinements are needed,
the ABCD score can be used in routine clinical practice to identify high-risk
individuals who need emergency investigation and treatment.
|