| Authors |
Dormandy
JA, Charbonnel B, Eckland DJ, Erdmann E, Massi-Benedetti M, Moules IK, Skene
AM, Tan MH, Lefebvre PJ, Murray GD, Standl E, Wilcox RG, Wilhelmsen L, Betteridge
J, Birkeland K, Golay A, Heine RJ, Koranyi L, Laakso M, Mokan M, Norkus
A, Pirags V, Podar T, Scheen A, Scherbaum W, Schernthaner G, Schmitz O,
Skrha J, Smith U, Taton J; PROactive investigators.
|
| Abstract |
BACKGROUND:
Patients with type 2 diabetes are at high risk of fatal and non-fatal
myocardial infarction and stroke. There is indirect evidence that agonists
of peroxisome proliferator-activated receptor gamma (PPAR gamma) could
reduce macrovascular complications. Our aim, therefore, was to ascertain
whether pioglitazone reduces macrovascular morbidity and mortality in
high-risk patients with type 2 diabetes.
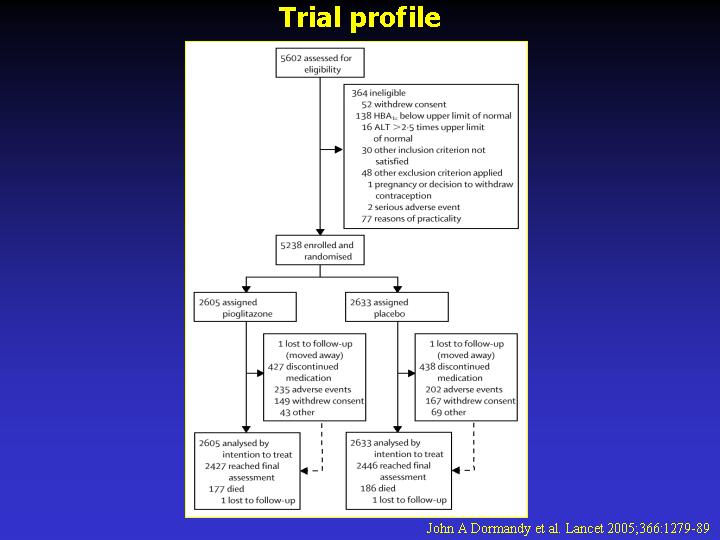
METHODS: We did a prospective, randomised controlled trial in 5238 patients
with type 2 diabetes who had evidence of macrovascular disease. We recruited
patients from primary-care practices and hospitals. We assigned patients
to oral pioglitazone titrated from 15 mg to 45 mg (n=2605) or matching
placebo (n=2633), to be taken in addition to their glucose-lowering drugs
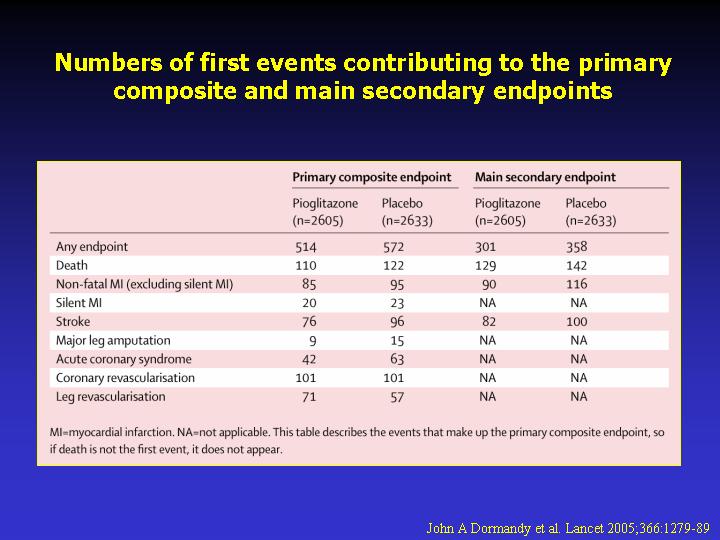
and other medications. Our primary endpoint was the composite of all-cause
mortality, non fatal myocardial infarction (including silent myocardial
infarction), stroke, acute coronary syndrome, endovascular or surgical
intervention in the coronary or leg arteries, and amputation above the
ankle. Analysis was by intention to treat. This study is registered as
an International Standard Randomised Controlled Trial, number ISRCTN NCT00174993.
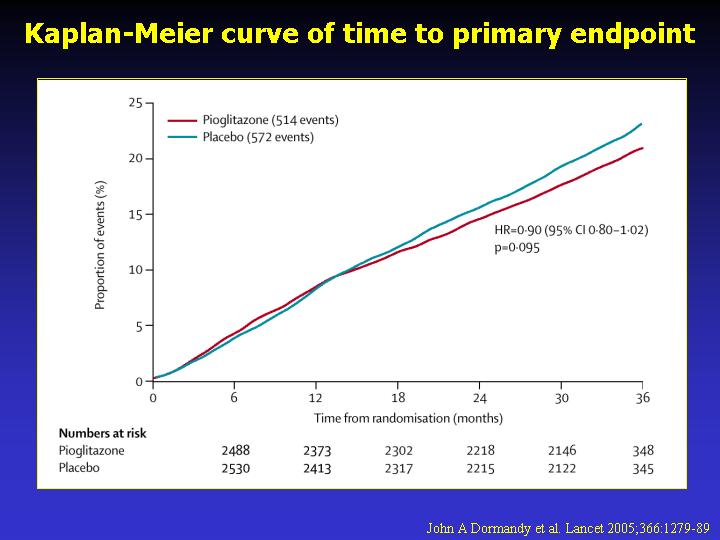
FINDINGS: Two patients were lost to follow-up, but were included in analyses.
The average time of observation was 34.5 months. 514 of 2605 patients
in the pioglitazone group and 572 of 2633 patients in the placebo group
had at least one event in the primary composite endpoint (HR 0.90, 95%
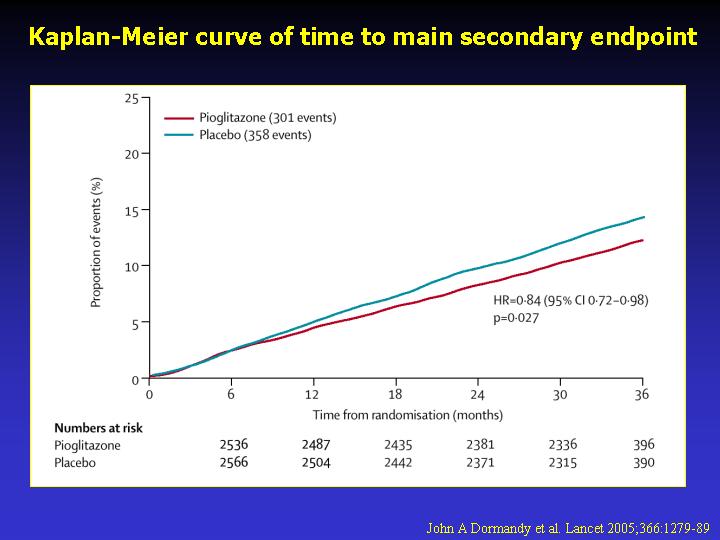
CI 0.80-1.02, p=0.095). The main secondary endpoint was the composite
of all-cause mortality, non-fatal myocardial infarction, and stroke. 301
patients in the pioglitazone group and 358 in the placebo group reached
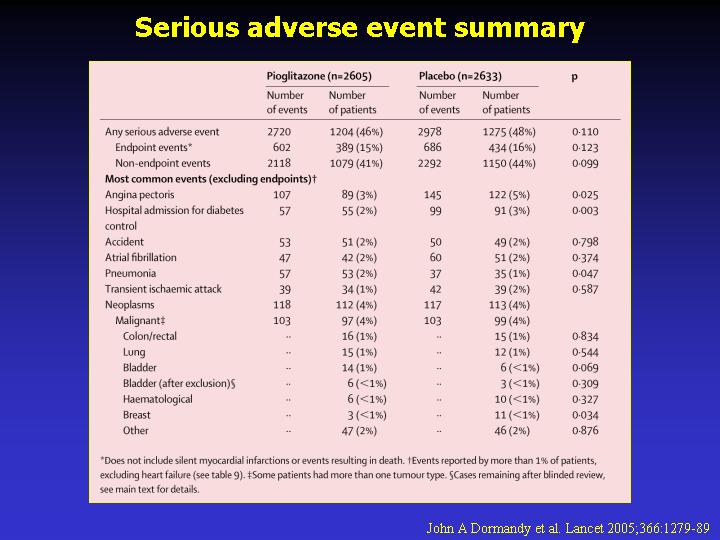
this endpoint (0.84, 0.72-0.98, p=0.027). Overall safety and tolerability
was good with no change in the safety profile of pioglitazone identified.
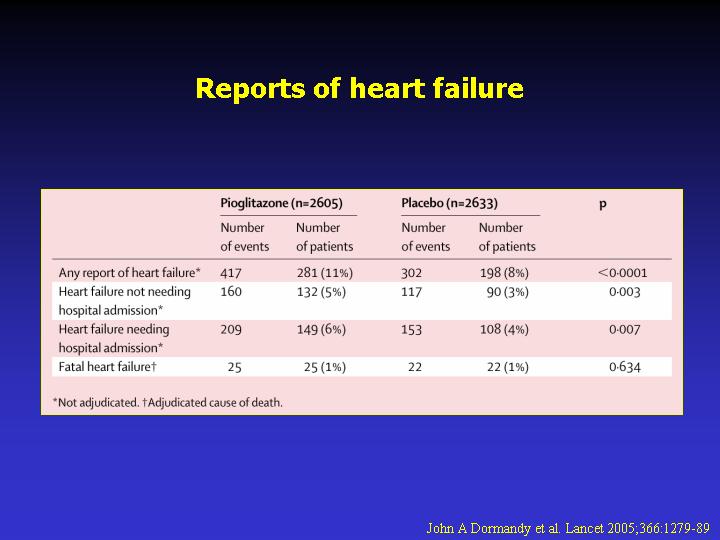
6% (149 of 2065) and 4% (108 of 2633) of those in the pioglitazone and
placebo groups, respectively, were admitted to hospital with heart failure;
mortality rates from heart failure did not differ between groups.
INTERPRETATION: Pioglitazone reduces the composite of all-cause mortality,
non-fatal myocardial infarction, and stroke in patients with type 2 diabetes
who have a high risk of macrovascular events.
|