| Authors |
Terje
R. Pedersen, MD, PhD; Ole Faergeman, MD, DMSc; John J. P. Kastelein, MD,
PhD; Anders G. Olsson, MD, PhD; Matti J. Tikkanen, MD, PhD; Ingar Holme,
PhD; Mogens Lytken Larsen, MD, DMSc; Fredrik S. Bendiksen, MD; Christina
Lindahl, MD; Michael Szarek, MS; John Tsai, MD; for the Incremental Decrease
in End Points Through Aggressive Lipid Lowering (IDEAL) Study Group
|
| Abstract |
Context
Evidence suggests that more intensive lowering of low-density lipoprotein
cholesterol (LDL-C) than is commonly applied clinically will provide further
benefit in stable coronary artery disease.
Objective To compare the effects of 2 strategies of lipid lowering
on the risk of cardiovascular disease among patients with a previous myocardial
infarction (MI).
Design, Setting, and Participants The IDEAL study, a prospective,
randomized, open-label, blinded end-point evaluation trial conducted at
190 ambulatory cardiology care and specialist practices in northern Europe
between March 1999 and March 2005 with a median follow-up of 4.8 years,
which enrolled 8888 patients aged 80 years or younger with a history of
acute MI.
Interventions Patients were randomly assigned to receive a high
dose of atorvastatin (80 mg/d; n = 4439), or usual-dose simvastatin (20
mg/d; n = 4449).
Main Outcome Measure Occurrence of a major coronary event, defined
as coronary death, confirmed nonfatal acute MI, or cardiac arrest with
resuscitation.
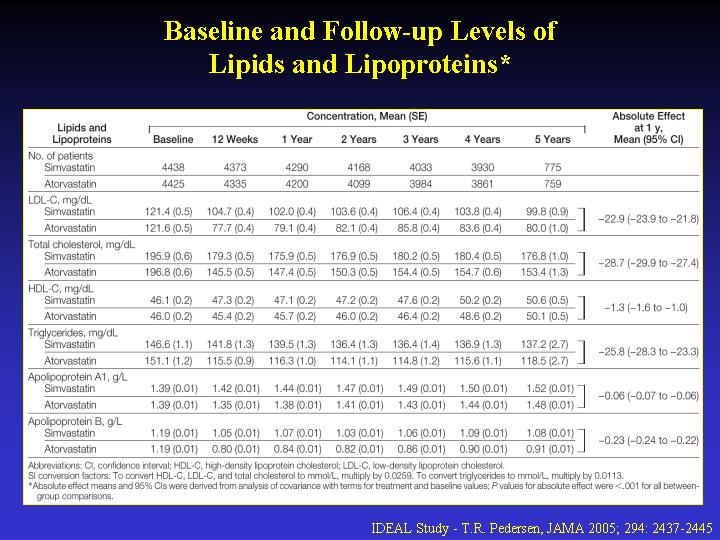
Results During treatment, mean LDL-C levels were 104 (SE, 0.3)
mg/dL in the simvastatin group and 81 (SE, 0.3) mg/dL in the atorvastatin
group. A major coronary event occurred in 463 simvastatin patients (10.4%)
and in 411 atorvastatin patients (9.3%) (hazard ratio [HR], 0.89; 95%
CI, 0.78-1.01; P = .07). Nonfatal acute MI occurred in 321 (7.2%) and
267 (6.0%) in the 2 groups (HR, 0.83; 95% CI, 0.71-0.98; P = .02), but
no differences were seen in the 2 other components of the primary end
point. Major cardiovascular events occurred in 608 and 533 in the 2 groups,
respectively (HR, 0.87; 95% CI, 0.77-0.98; P = .02). Occurrence of any
coronary event was reported in 1059 simvastatin and 898 atorvastatin patients
(HR, 0.84; 95% CI, 0.76-0.91; P<.001). Noncardiovascular death occurred
in 156 (3.5%) and 143 (3.2%) in the 2 groups (HR, 0.92; 95% CI, 0.73-1.15;
P = .47). Death from any cause occurred in 374 (8.4%) in the simvastatin
group and 366 (8.2%) in the atorvastatin group (HR, 0.98; 95% CI, 0.85-1.13;
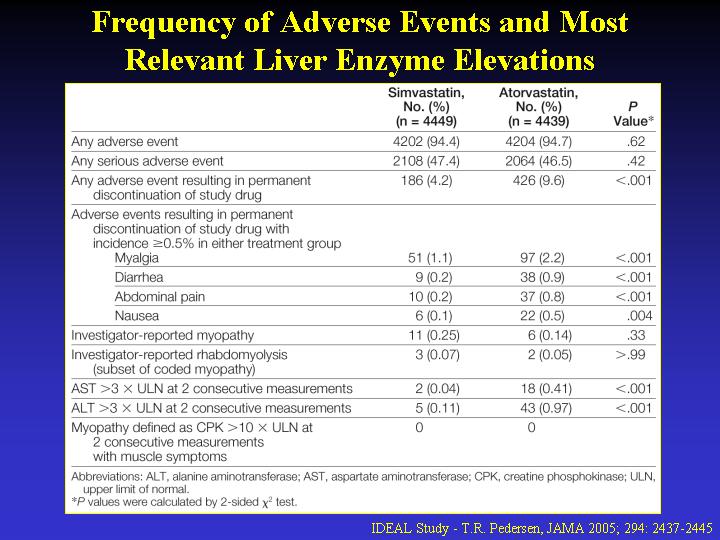
P = .81). Patients in the atorvastatin group had higher rates of drug
discontinuation due to nonserious adverse events; transaminase elevation
resulted in 43 (1.0%) vs 5 (0.1%) withdrawals (P<.001). Serious myopathy
and rhabdomyolysis were rare in both groups.
Conclusions In this study of patients with previous MI, intensive
lowering of LDL-C did not result in a significant reduction in the primary
outcome of major coronary events, but did reduce the risk of other composite
secondary end points and nonfatal acute MI. There were no differences
in cardiovascular or all-cause mortality. Patients with MI may benefit
from intensive lowering of LDL-C without an increase in noncardiovascular
mortality or other serious adverse reactions
|