| Authors |
Grover
SA, Lowensteyn I, Kaouache M, Marchand S, Coupal L, DeCarolis E, Zoccoli
J, Defoy I.
|
| Abstract |
BACKGROUND:
The prevalence of erectile dysfunction (ED) and associated risk factors
has been described in many clinical settings, but there is little information
regarding men seen by primary care physicians. We sought to identify independent
factors associated with ED in a primary care setting.
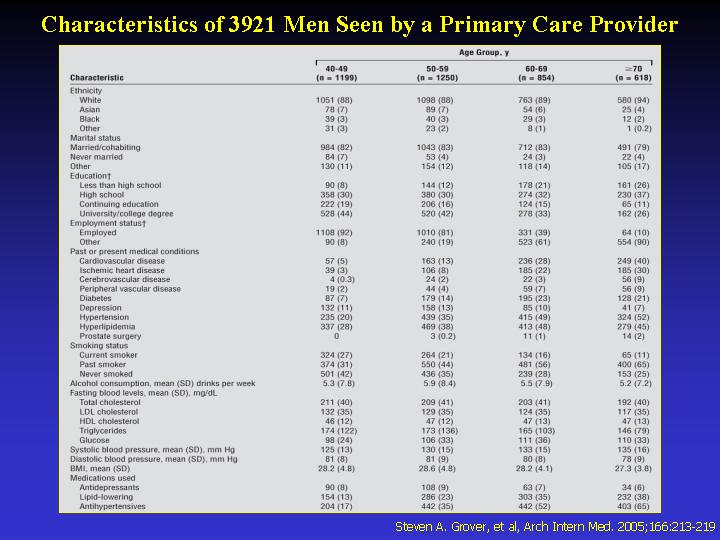
METHODS: We surveyed a cross-sectional sample of 3921 Canadian men, aged
40 to 88 years, seen by primary care physicians. Participants completed
a full medical history, physical examination, and measurement of fasting
blood glucose and lipid levels. We used the International Index of Erectile
Function to define ED as a score of less than 26 on the erectile function
domain.
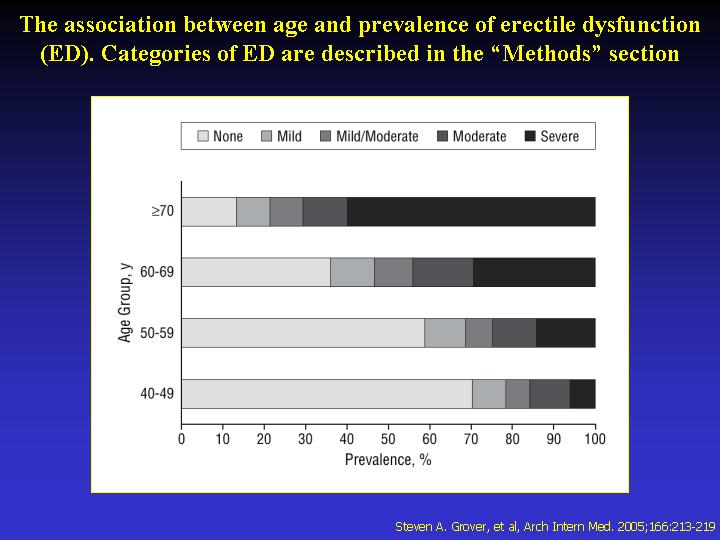
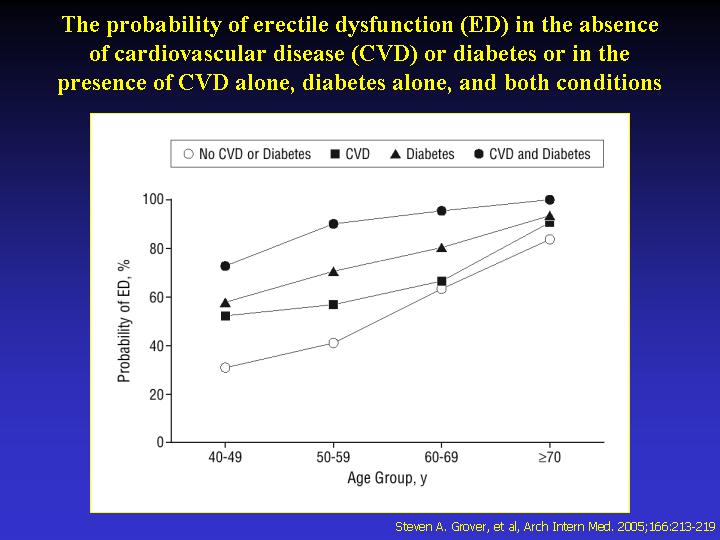
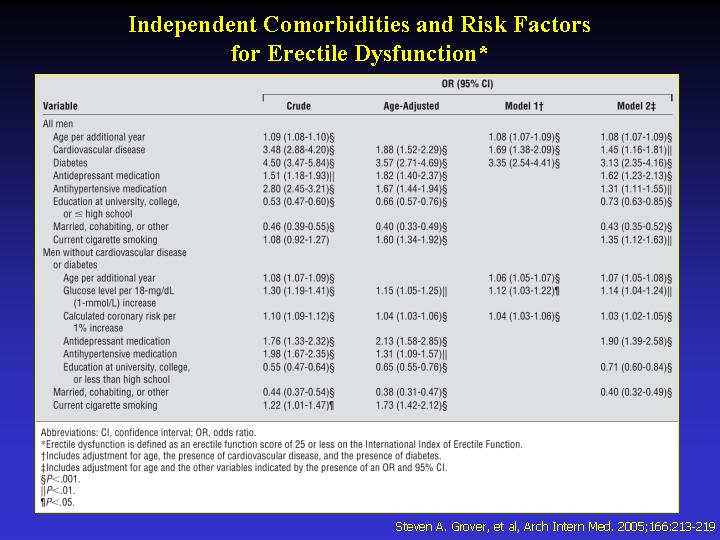
RESULTS: The overall prevalence of ED was 49.4%. The presence of cardiovascular
disease (odds ratio [OR], 1.45; 95% confidence interval [CI], 1.16-1.81;
P<.01) or diabetes (OR, 3.13; 95% CI, 2.35-4.16; P<.001) increased
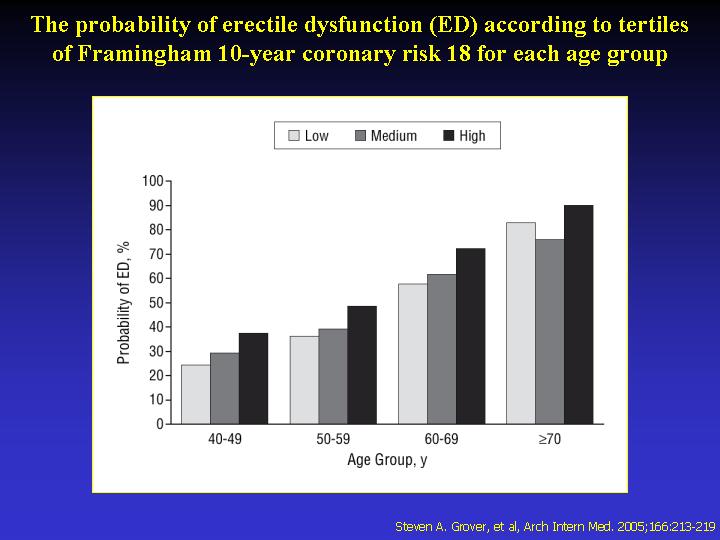
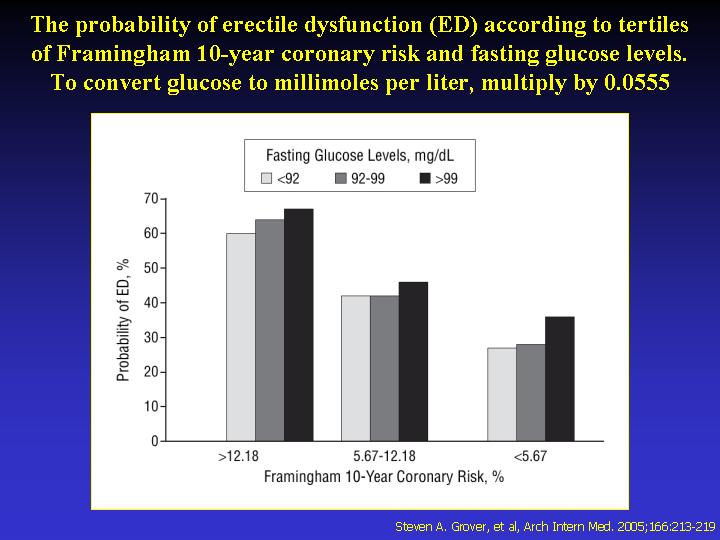
the probability of ED after adjustment for other confounders. Among those
individuals without cardiovascular disease or diabetes, the calculated
10-year Framingham coronary risk (OR, 1.03 per 1% increase; 95% CI, 1.02-1.05;
P<.001) and fasting blood glucose levels (OR, 1.14 per 18-mg/dL [1-mmol/L]
increase; 95% CI, 1.04-1.24; P<.01) were independently associated with
ED. Erectile dysfunction was also independently associated with undiagnosed
hyperglycemia (OR, 1.46; 95% CI, 1.02-2.10; P = .04), impaired fasting
glucose (OR, 1.26; 95% CI, 1.08-1.46; P = .004), and the metabolic syndrome
(OR, 1.45; 95% CI, 1.24-1.69; P<.001).
CONCLUSIONS: Cardiovascular disease, diabetes, future coronary risk, and
increasing fasting glucose levels are independently associated with ED.
It remains to be determined if ED precedes the development of these conditions.
|