| Abstract |
BACKGROUND:
A low ankle-arm index (AAI) is a strong predictor of mortality and cardiovascular
events. A high AAI also appears to be associated with higher mortality
risk in select populations. However, mortality and cardiovascular risk
across the AAI spectrum have not been described in a more broadly defined
population.
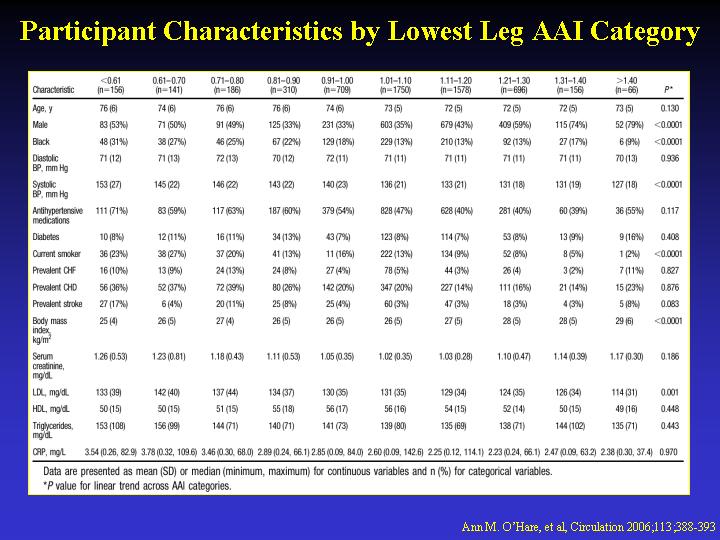
METHODS AND RESULTS: We examined total and cardiovascular mortality and
cardiovascular events across the AAI spectrum among 5748 participants
in the Cardiovascular Health Study (CHS). The mean age of the sample population
was 73+/-6 years, and the sample included 3289 women (57%) and 883 blacks
(15%). The median duration of follow-up was 11.1 (0.1 to 12) years for
mortality and 9.6 (0.1 to 12.1) years for cardiovascular events. There
were 2311 deaths (953 of which were cardiovascular) and 1491 cardiovascular
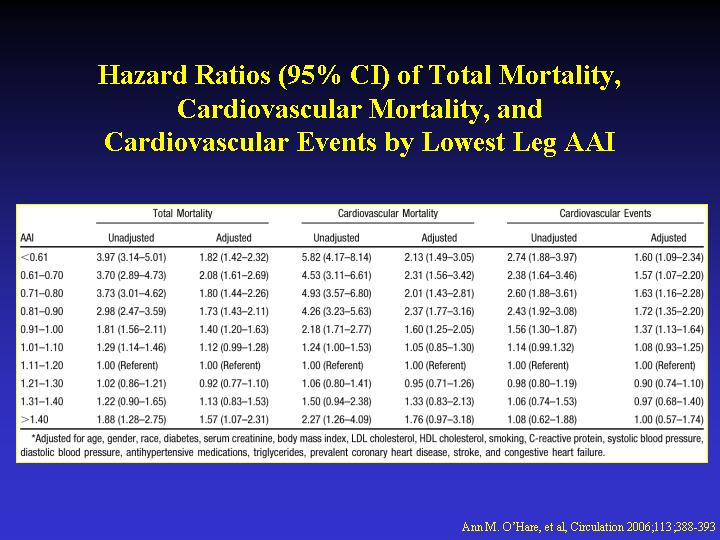
events during follow-up. After adjustment for potential confounders, AAI
measurements < or =0.60 (hazard ratio [HR] 1.82, 95% CI 1.42 to 2.32),
0.61 to 0.7 (HR 2.08, 95% CI 1.61 to 2.69), 0.71 to 0.8 (HR 1.80, 95%
CI 1.44 to 2.26), 0.81 to 0.9 (HR 1.73 95% CI 1.43 to 2.11), 0.91 to 1.0
(HR 1.40, 95% CI 1.20 to 1.63), and >1.40 (HR 1.57, 95% CI 1.07 to
2.31) were associated with higher mortality risk from all causes compared
with the referent group (AAI 1.11 to 1.20). The pattern was similar for
cardiovascular mortality. For cardiovascular events, risk was higher at
all AAI levels <1 but not for AAI levels >1.4 (HR 1.00, 95% CI 0.57
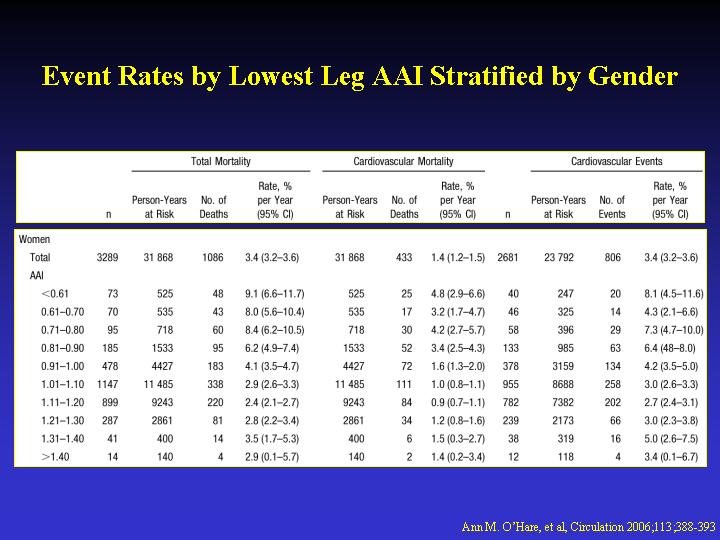
to 1.74). The association of a high AAI with mortality was stronger in
men than in women and in younger than in older cohort members.
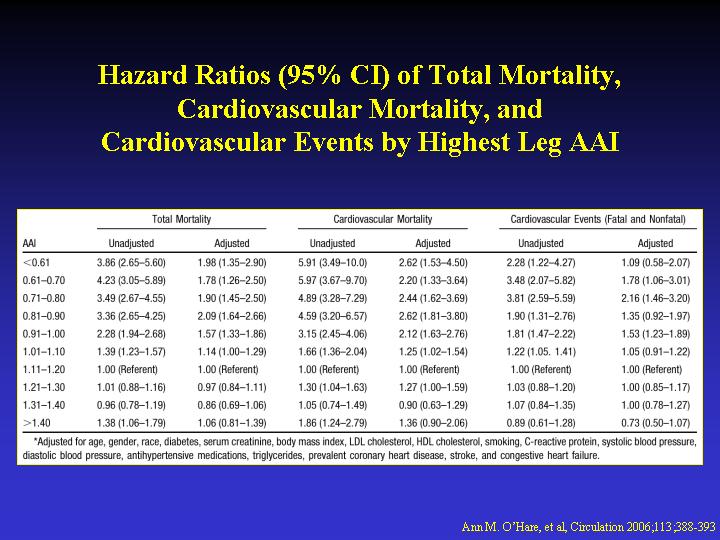
CONCLUSIONS: In a cohort of community-dwelling elders, mortality risk
was higher than the referent category of 1.11 to 1.2 among participants
with AAI values above the traditional cutpoint of 0.9 (ie, 0.91 to 1.0
and >1.4), and the specific association of AAI with mortality varied
by age and gender
|