| Abstract |
BACKGROUND:
Atherosclerosis and sepsis share several pathophysiological similarities,
including immune dysregulation, increased thrombogenesis, and systemic
inflammation. The relation between statins and risk of sepsis in patients
with atherosclerosis is unknown.
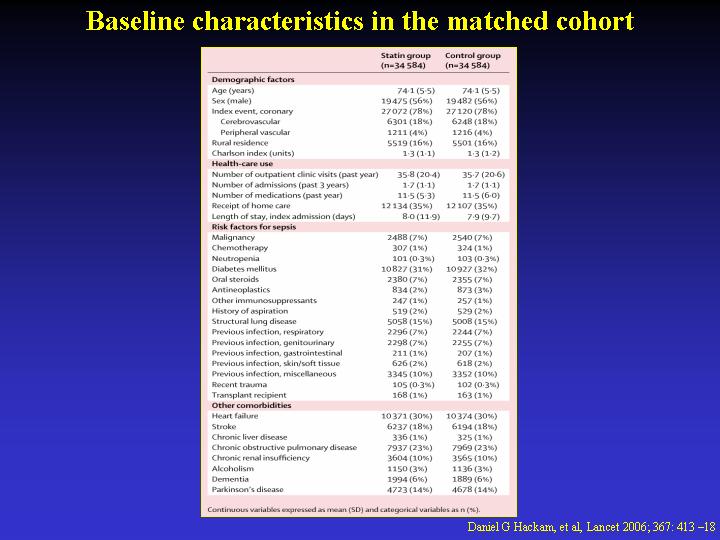
METHODS: We did a population-based cohort analysis through linked administrative
databases in Ontario, Canada, with accrual from 1997 to 2002. We identified
141,487 patients older than 65 years who had been hospitalised for an
acute coronary syndrome, ischaemic stroke, or revascularisation, who survived
for at least 3 months after discharge. 46,662 (33%) were prescribed a
statin within 90 days of discharge, 94,825 (67%) were not. Propensity-based
matching, which accounted for each individual's likelihood of receiving
a statin, yielded a cohort of 69,168 patients, of whom half (34,584) received
a statin and half (34,584) did not.
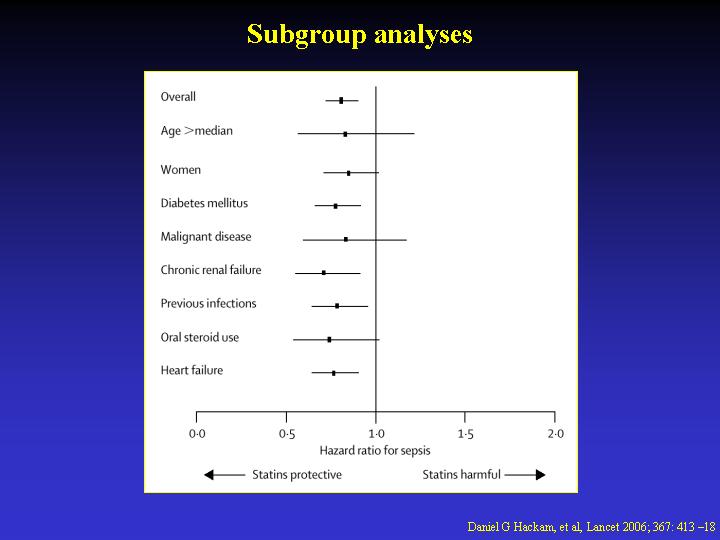
FINDINGS: Incidence of sepsis was lower in patients receiving statins
than in controls (71.2 vs 88.0 events per 10,000 person-years; hazard
ratio [HR] 0.81; 95% CI 0.72-0.91). Adjustment for demographic characteristics,
sepsis risk factors, comorbidities, and health-care use gave similar results
(HR 0.81; 95% CI 0.72-0.90). The protective association between statins
and sepsis persisted in high-risk subgroups, including patients with diabetes
mellitus, chronic renal failure, or a history of infections. Significant
reductions in severe sepsis (HR 0.83; 95% CI 0.70-0.97) and fatal sepsis
(0.75; 0.61-0.93) were also observed. No benefit was noted with non-statin
lipid-lowering agents (0.95; 0.75-1.22).
IMPLICATIONS: Use of statins in patients with atherosclerosis is associated
with a reduced risk of subsequent sepsis. Randomised trials of statins
for prevention of sepsis are warranted.
|