| Authors |
Nissen
SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, Davignon
J, Erbel R, Fruchart JC, Tardif JC, Schoenhagen P, Crowe T, Cain V, Wolski
K, Goormastic M, Tuzcu EM.
|
| Abstract |
CONTEXT:
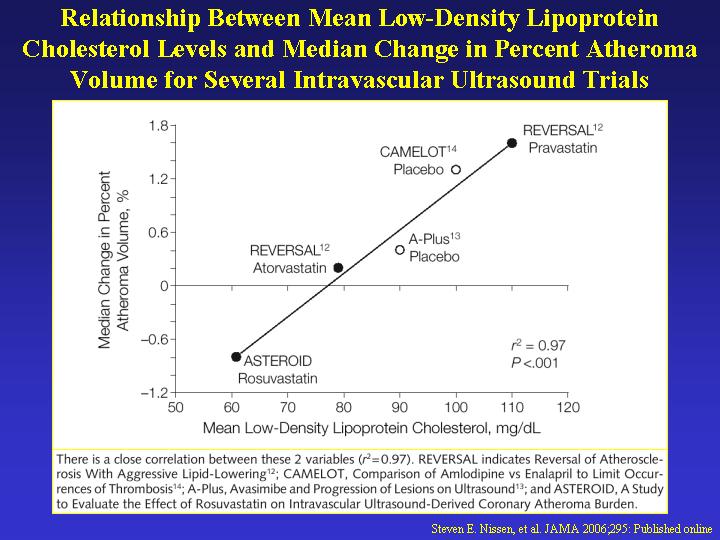
Prior intravascular ultrasound (IVUS) trials have demonstrated slowing
or halting of atherosclerosis progression with statin therapy but have
not shown convincing evidence of regression using percent atheroma volume
(PAV), the most rigorous IVUS measure of disease progression and regression.
OBJECTIVE: To assess whether very intensive statin therapy could regress
coronary atherosclerosis as determined by IVUS imaging.
DESIGN AND SETTING: Prospective, open-label blinded end-points trial (A
Study to Evaluate the Effect of Rosuvastatin on Intravascular Ultrasound-Derived
Coronary Atheroma Burden [ASTEROID]) was performed at 53 community and
tertiary care centers in the United States, Canada, Europe, and Australia.
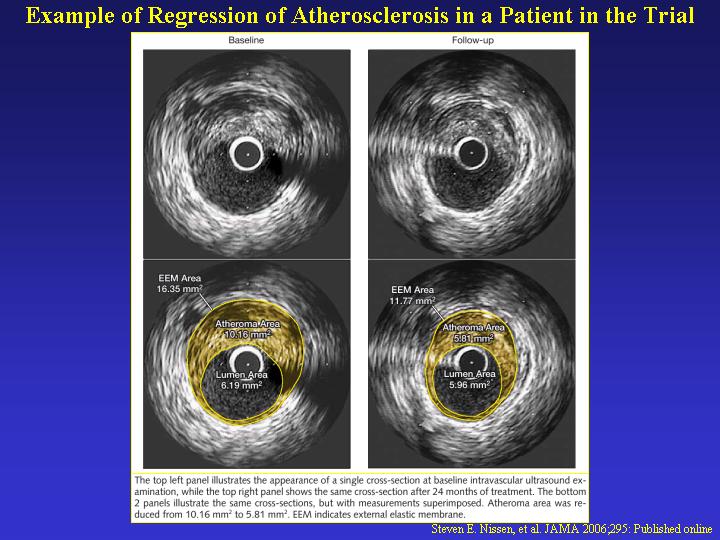
A motorized IVUS pullback was used to assess coronary atheroma burden
at baseline and after 24 months of treatment. Each pair of baseline and
follow-up IVUS assessments was analyzed in a blinded fashion.
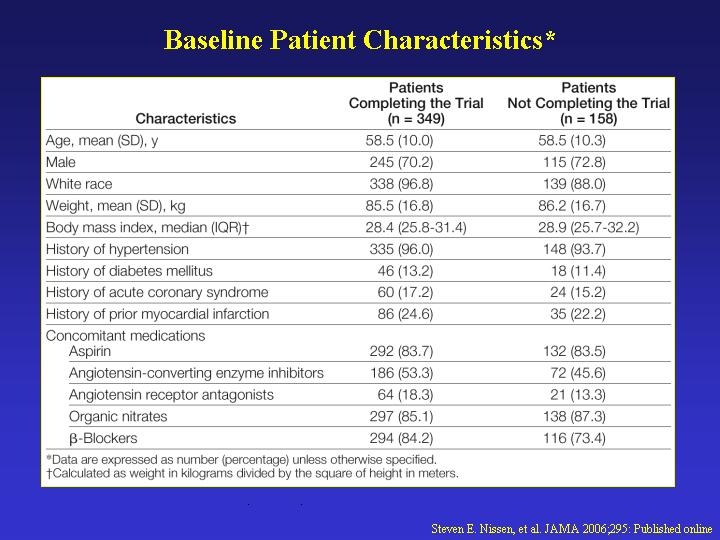
PATIENTS: Between November 2002 and October 2003, 507 patients had a baseline
IVUS examination and received at least 1 dose of study drug. After 24
months, 349 patients had evaluable serial IVUS examinations.
INTERVENTION: All patients received intensive statin therapy with rosuvastatin,
40 mg/d.
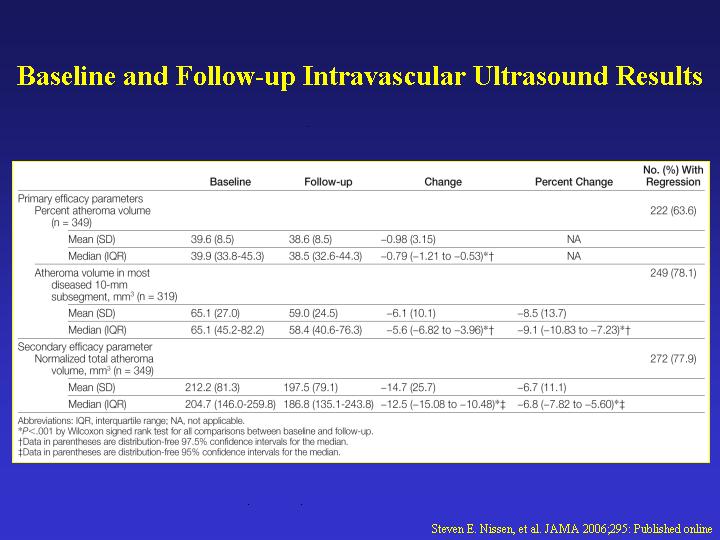
MAIN OUTCOME MEASURES: Two primary efficacy parameters were prespecified:
the change in PAV and the change in nominal atheroma volume in the 10-mm
subsegment with the greatest disease severity at baseline. A secondary
efficacy variable, change in normalized total atheroma volume for the
entire artery, was also prespecified.
RESULTS: The mean (SD) baseline low-density lipoprotein cholesterol (LDL-C)
level of 130.4 (34.3) mg/dL declined to 60.8 (20.0) mg/dL, a mean reduction
of 53.2% (P<.001). Mean (SD) high-density lipoprotein cholesterol (HDL-C)
level at baseline was 43.1 (11.1) mg/dL, increasing to 49.0 (12.6) mg/dL,
an increase of 14.7% (P<.001). The mean (SD) change in PAV for the
entire vessel was -0.98% (3.15%), with a median of -0.79% (97.5% CI, -1.21%
to -0.53%) (P<.001 vs baseline). The mean (SD) change in atheroma volume
in the most diseased 10-mm subsegment was -6.1 (10.1) mm(3), with a median
of -5.6 mm(3) (97.5% CI, -6.8 to -4.0 mm(3)) (P<.001 vs baseline).
Change in total atheroma volume showed a 6.8% median reduction; with a
mean (SD) reduction of -14.7 (25.7) mm(3), with a median of -12.5 mm(3)
(95% CI, -15.1 to -10.5 mm(3)) (P<.001 vs baseline). Adverse events
were infrequent and similar to other statin trials. CONCLUSIONS: Very
high-intensity statin therapy using rosuvastatin 40 mg/d achieved an average
LDL-C of 60.8 mg/dL and increased HDL-C by 14.7%, resulting in significant
regression of atherosclerosis for all 3 prespecified IVUS measures of
disease burden. Treatment to LDL-C levels below currently accepted guidelines,
when accompanied by significant HDL-C increases, can regress atherosclerosis
in coronary disease patients. Further studies are needed to determine
the effect of the observed changes on clinical outcome.Trial Registration
ClinicalTrials.gov Identifier: NCT00240318
|