| Authors |
Bonaa
KH, Njolstad I, Ueland PM, Schirmer H, Tverdal A, Steigen T, Wang H, Nordrehaug
JE, Arnesen E, Rasmussen K; NORVIT Trial Investigators.
|
| Abstract |
BACKGROUND:
Homocysteine is a risk factor for cardiovascular disease. We evaluated
the efficacy of homocysteine-lowering treatment with B vitamins for secondary
prevention in patients who had had an acute myocardial infarction.
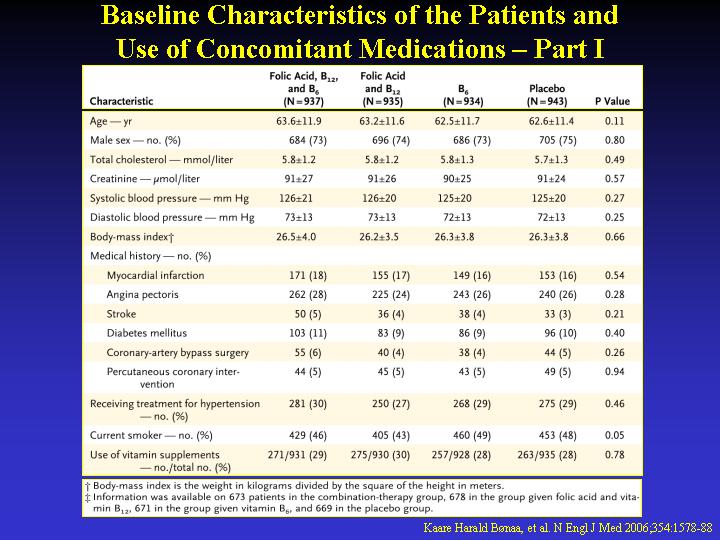
METHODS: The trial included 3749 men and women who had had an acute myocardial
infarction within seven days before randomization. Patients were randomly
assigned, in a two-by-two factorial design, to receive one of the following
four daily treatments: 0.8 mg of folic acid, 0.4 mg of vitamin B12, and
40 mg of vitamin B6; 0.8 mg of folic acid and 0.4 mg of vitamin B12; 40
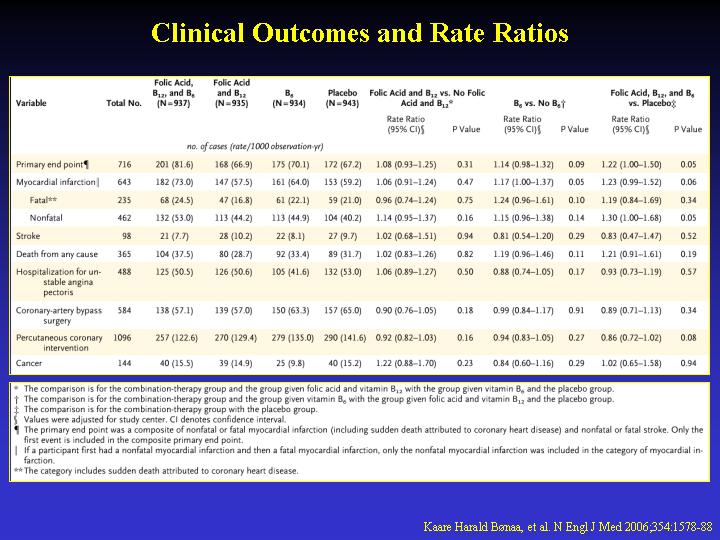
mg of vitamin B6; or placebo. The primary end point during a median follow-up
of 40 months was a composite of recurrent myocardial infarction, stroke,
and sudden death attributed to coronary artery disease.
RESULTS: The mean total homocysteine level was lowered by 27 percent among
patients given folic acid plus vitamin B12, but such treatment had no
significant effect on the primary end point (risk ratio, 1.08; 95 percent
confidence interval, 0.93 to 1.25; P=0.31). Also, treatment with vitamin
B6 was not associated with any significant benefit with regard to the
primary end point (relative risk of the primary end point, 1.14; 95 percent
confidence interval, 0.98 to 1.32; P=0.09). In the group given folic acid,
vitamin B12, and vitamin B6, there was a trend toward an increased risk
(relative risk, 1.22; 95 percent confidence interval, 1.00 to 1.50; P=0.05).
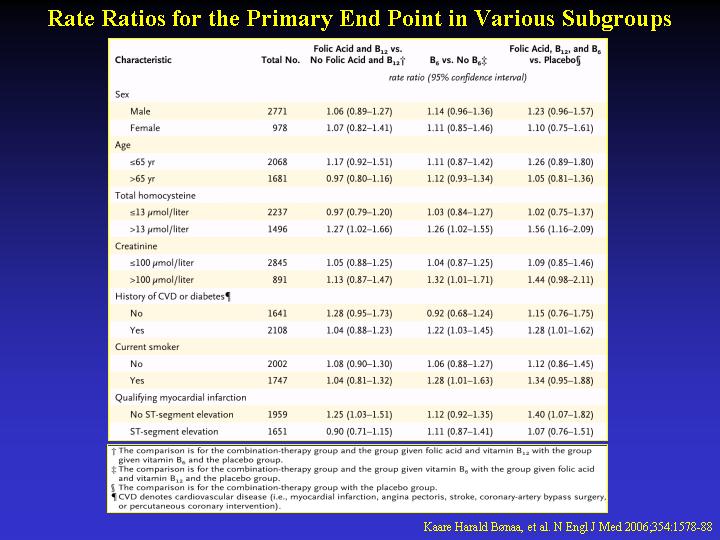
CONCLUSIONS: Treatment with B vitamins did not lower the risk of recurrent
cardiovascular disease after acute myocardial infarction. A harmful effect
from combined B vitamin treatment was suggested. Such treatment should
therefore not be recommended. (ClinicalTrials.gov number, NCT00266487).
|