| Authors |
Sabatine MS, Morrow DA, Jablonski KA, Rice MM, Warnica JW, Domanski MJ, Hsia J, Gersh BJ, Rifai N, Ridker PM, Pfeffer MA, Braunwald E; PEACE Investigators. |
|
| Title |
Prognostic significance of the Centers for Disease Control/American Heart Association high-sensitivity C-reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease |
|
| Full source | Circulation 2007;115:1528-36 | |
|
|
Per scorrere le diapositive |
|
|
||
| Abstract |
BACKGROUND:
Data supporting the prognostic significance of high-sensitivity C-reactive
protein (hs-CRP) are derived largely from individuals with no overt coronary
artery disease or from patients with acute coronary syndromes. In contrast,
the ability of hs-CRP to predict outcomes in patients with stable coronary
artery disease and the prognostic significance of the Centers for Disease
Control/American Heart Association hs-CRP cut points in such a population
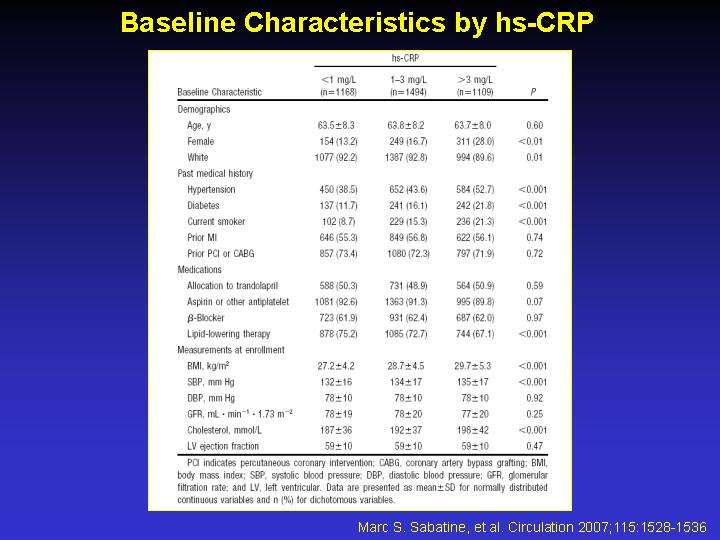
remain relatively unexplored. METHODS AND RESULTS: We measured hs-CRP
in 3771 patients with stable coronary artery disease from the Prevention
of Events With Angiotensin-Converting Enzyme Inhibition (PEACE) trial,
a randomized placebo-controlled trial of the angiotensin-converting enzyme
inhibitor trandolapril. Patients were followed up for a median of 4.8
years for cardiovascular death, myocardial infarction, or stroke, as well
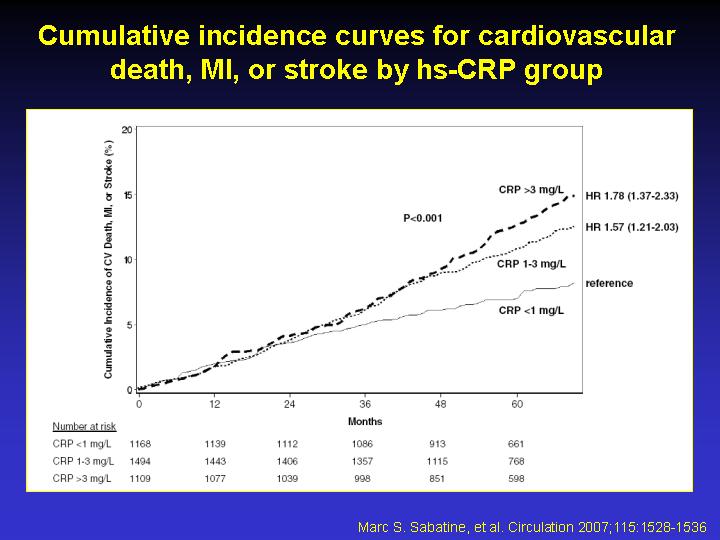
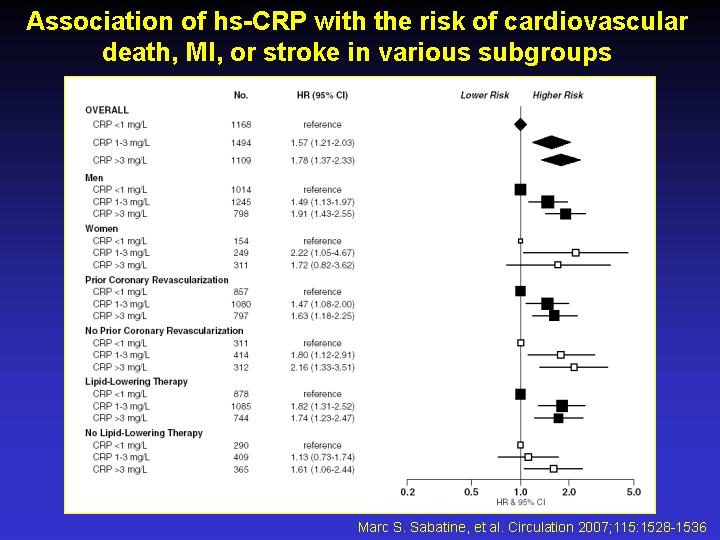
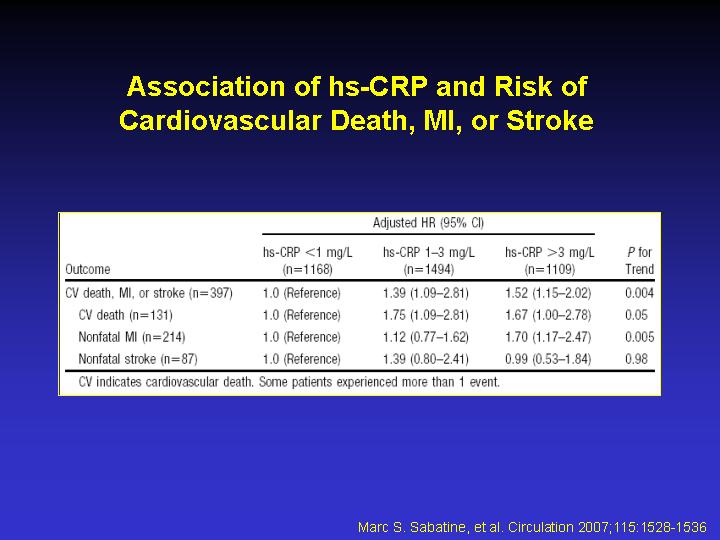
as new heart failure and diabetes. After adjustment for baseline characteristics
and treatments, higher hs-CRP levels, even >1 mg/L, were associated
with a significantly greater risk of cardiovascular death, myocardial
infarction, or stroke (hs-CRP 1 to 3 mg/L: adjusted hazard ratio, 1.39;
95% CI, 1.06 to 1.81; P=0.016; hs-CRP >3 mg/L: adjusted hazard ratio,
1.52; 95% CI, 1.15 to 2.02; P=0.003). Similarly, elevated hs-CRP levels
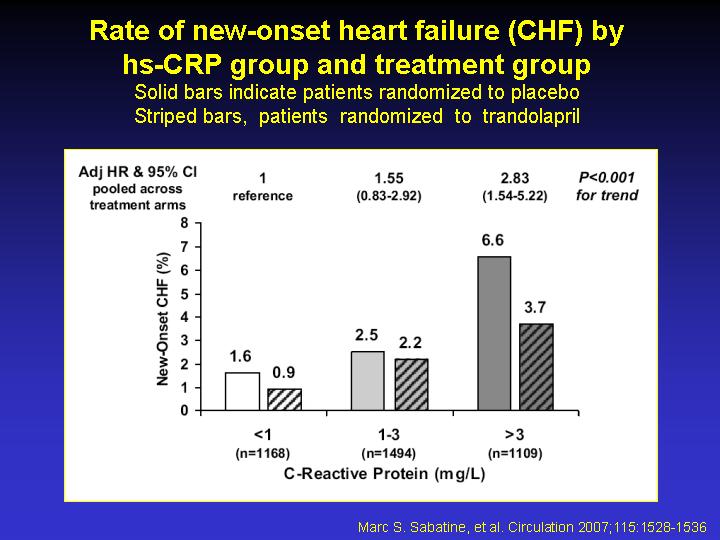
were an independent predictor of new heart failure (adjusted P<0.001
for trend) and new diabetes (adjusted P<0.001 for trend). There were
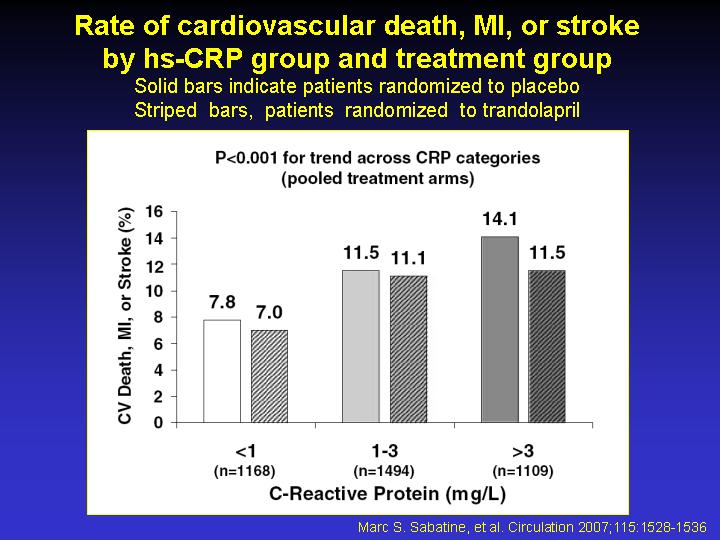
no significant interactions between hs-CRP levels and the effects of trandolapril
on any of the above outcomes. CONCLUSIONS: In stable coronary artery disease,
an elevated hs-CRP level, even >1 mg/L, is a significant predictor
of adverse cardiovascular events independently of baseline characteristics
and treatments. An elevated hs-CRP does not appear to identify patients
with stable coronary artery disease and preserved ejection fraction who
derive particular benefit from angiotensin-converting enzyme inhibition. |
|