| Authors |
Emerging
Risk Factors Collaboration, Erqou S, Kaptoge S, Perry PL, Di Angelantonio
E, Thompson A, White IR, Marcovina SM, Collins R, Thompson SG, Danesh
J.
|
| Abstract
|
CONTEXT
Circulating concentration of lipoprotein(a) (Lp[a]), a large glycoprotein
attached to a low-density lipoprotein-like particle, may be associated
with risk of coronary heart disease (CHD) and stroke.
OBJECTIVE To assess the relationship of Lp(a) concentration with risk
of major vascular and nonvascular outcomes.
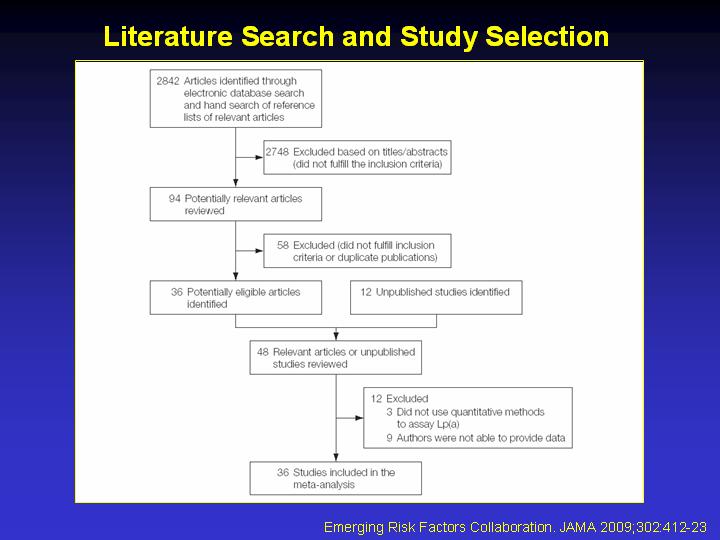
STUDY SELECTION Long-term prospective studies that recorded Lp(a) concentration
and subsequent major vascular morbidity and/or cause-specific mortality
published between January 1970 and March 2009 were identified through
electronic searches of MEDLINE and other databases, manual searches of
reference lists, and discussion with collaborators.
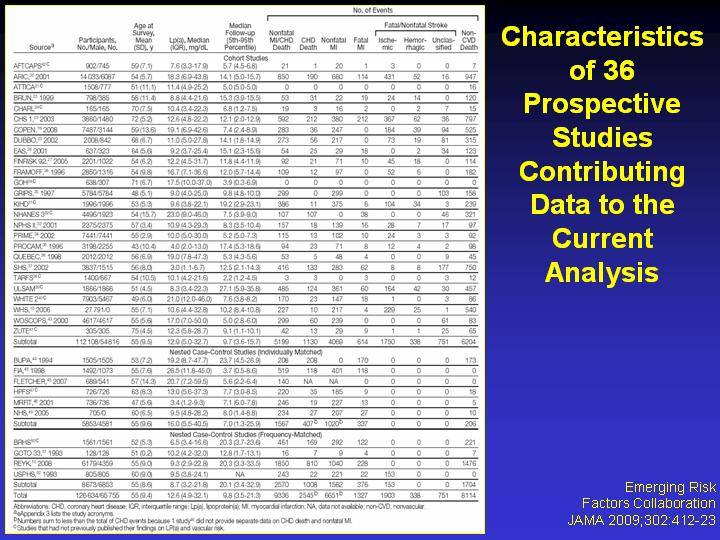
DATA EXTRACTION Individual records were provided for each of 126 634 participants
in 36 prospective studies. During 1.3 million person-years of follow-up,
22 076 firstever fatal or nonfatal vascular disease outcomes or nonvascular
deaths were recorded, including 9336 CHD outcomes, 1903 ischemic strokes,
338 hemorrhagic strokes, 751 unclassified strokes, 1091 other vascular
deaths, 8114 nonvascular deaths, and 242 deaths of unknown cause. Within-study
regression analyses were adjusted for within-person variation and combined
using meta-analysis. Analyses excluded participants with known preexisting
CHD or stroke at baseline.
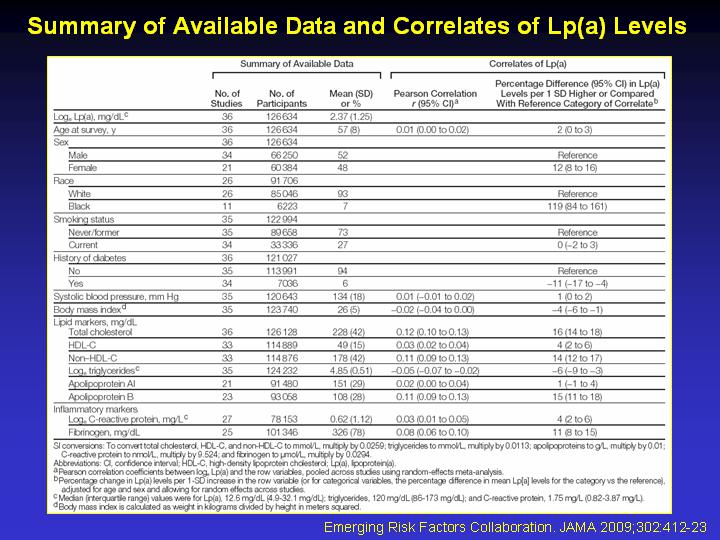
DATA SYNTHESIS Lipoprotein(a) concentration was weakly correlated with
several conventional vascular risk factors and it was highly consistent
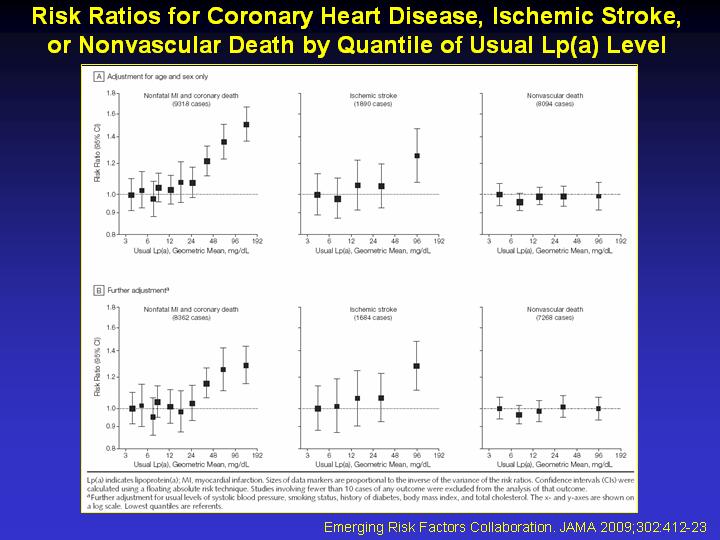
within individuals over several years. Associations of Lp(a) with CHD
risk were broadly continuous in shape. In the 24 cohort studies, the rates
of CHD in the top and bottom thirds of baseline Lp(a) distributions, respectively,
were 5.6 (95% confidence interval [CI], 5.4-5.9) per 1000 personyears
and 4.4 (95% CI, 4.2-4.6) per 1000 person-years. The risk ratio for CHD,
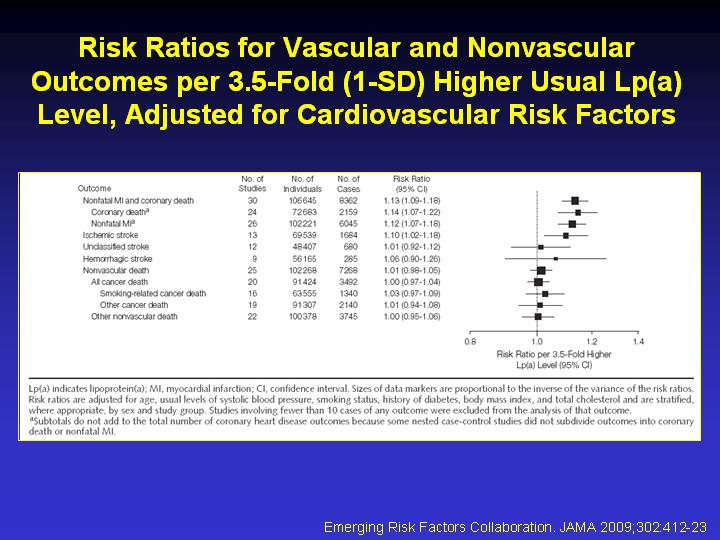
adjusted for age and sex only, was 1.16 (95% CI, 1.11-1.22) per 3.5-fold
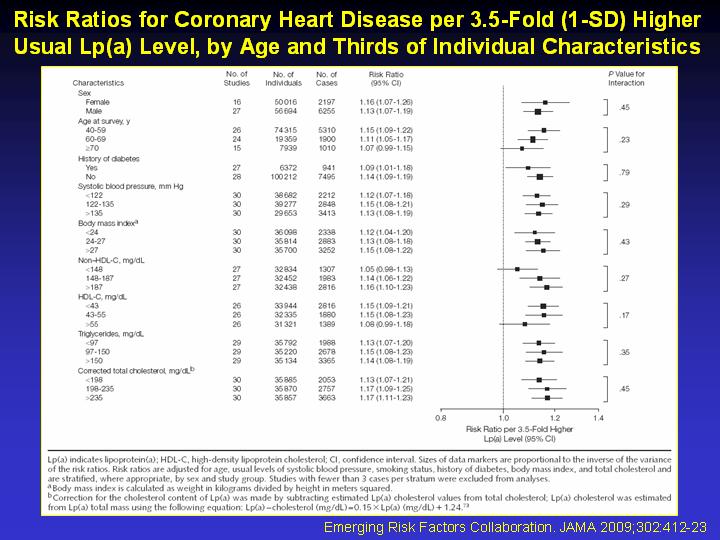
higher usual Lp(a) concentration (ie, per 1 SD), and it was 1.13 (95%
CI, 1.09-1.18) following further adjustment for lipids and other conventional
risk factors. The corresponding adjusted risk ratios were 1.10 (95% CI,
1.02-1.18) for ischemic stroke, 1.01 (95% CI, 0.98-1.05) for the aggregate
of nonvascular mortality, 1.00 (95% CI, 0.97-1.04) for cancer deaths,
and 1.00 (95% CI, 0.95-1.06) for nonvascular deaths other than cancer.
CONCLUSION Under a wide range of circumstances, there are continuous,
independent, and modest associations of Lp(a) concentration with risk
of CHD and stroke that appear exclusive to vascular outcomes.
|