| |
|
| Authors |
Nordestgaard
BG, Chapman MJ, Ray K, Borén J, Andreotti F, Watts GF,
Ginsberg H, Amarenco P, Catapano A, Descamps OS, Fisher E, Kovanen
PT, Kuivenhoven JA, Lesnik P, Masana L, Reiner Z, Taskinen MR,
Tokgözoglu L, Tybjærg-Hansen A; European Atherosclerosis
Society Consensus Panel.
|
| Title |
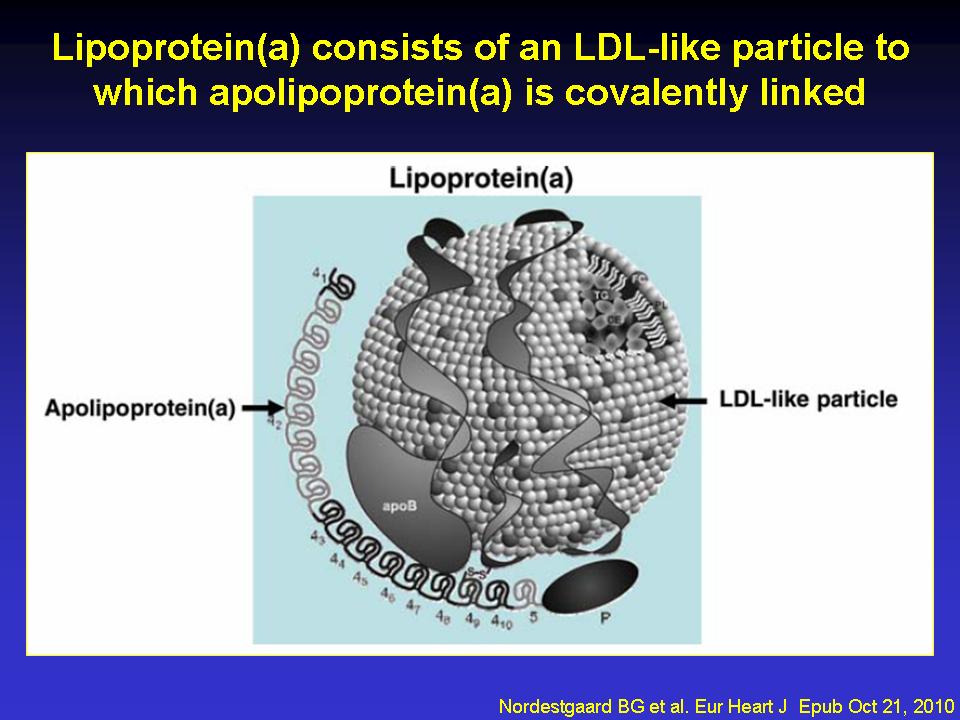
Lipoprotein(a)
as a cardiovascular risk factor: current status
|
| Full
source |
Eur Heart J 2010;31:2844-53 |
|
|

Per scorrere le diapositive
|
|
| Abstract
|
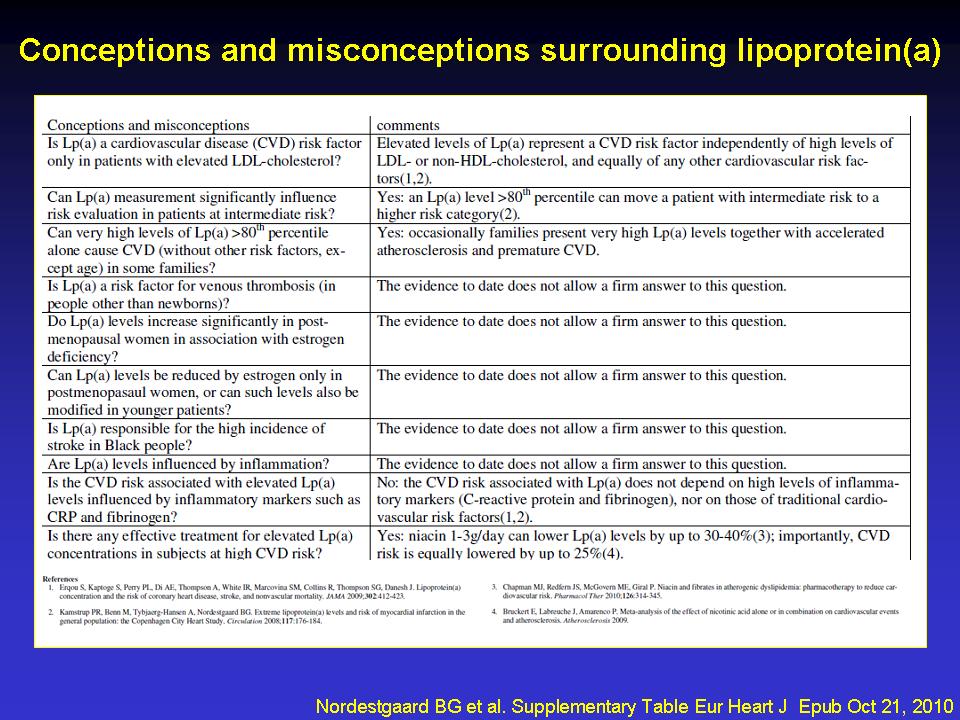
AIMS: The aims of the study were, first, to critically evaluate
lipoprotein(a) [Lp(a)] as a cardiovascular risk factor and, second,
to advise on screening for elevated plasma Lp(a), on desirable
levels, and on therapeutic strategies.
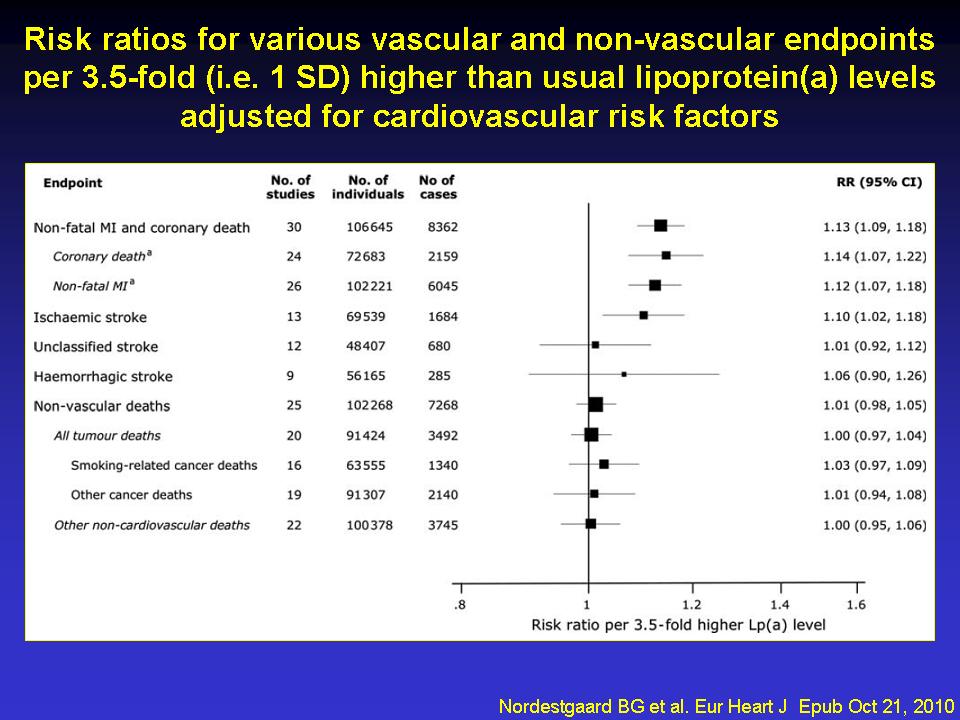
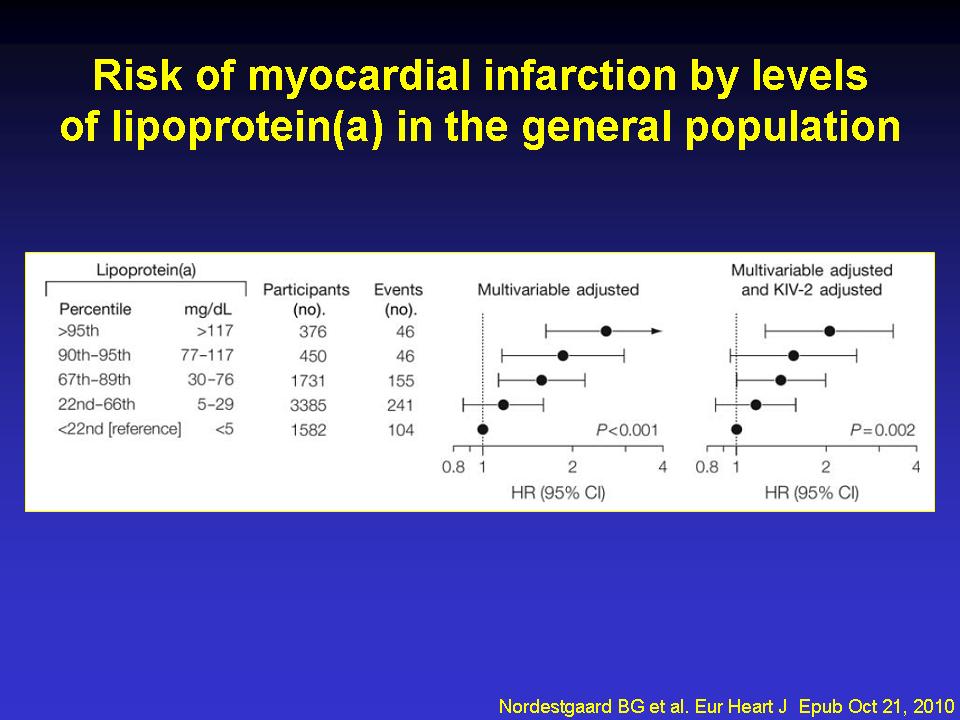
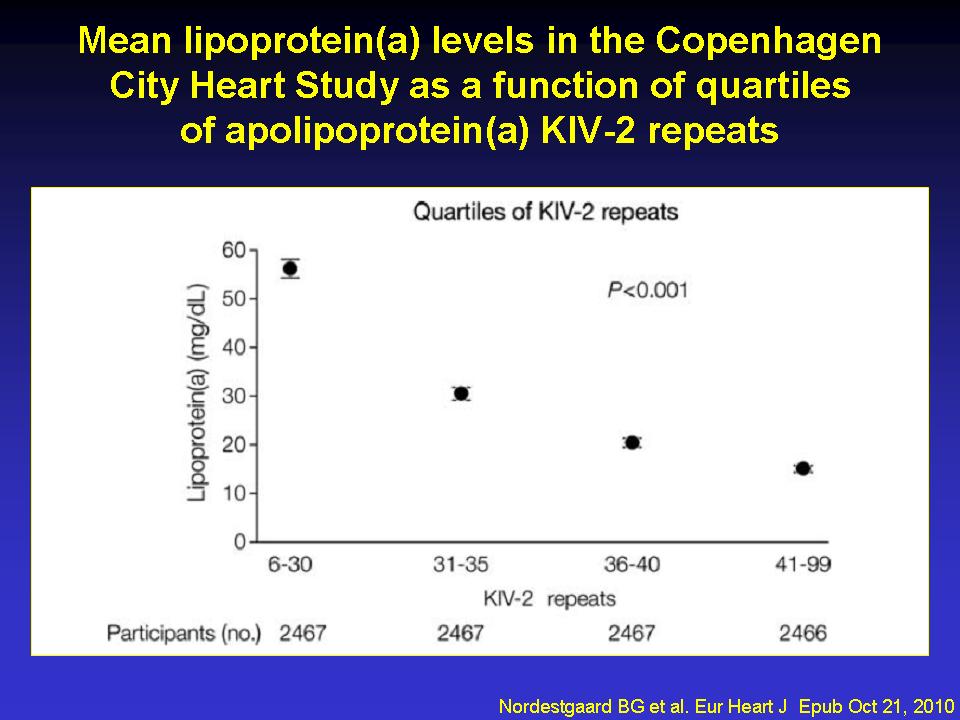
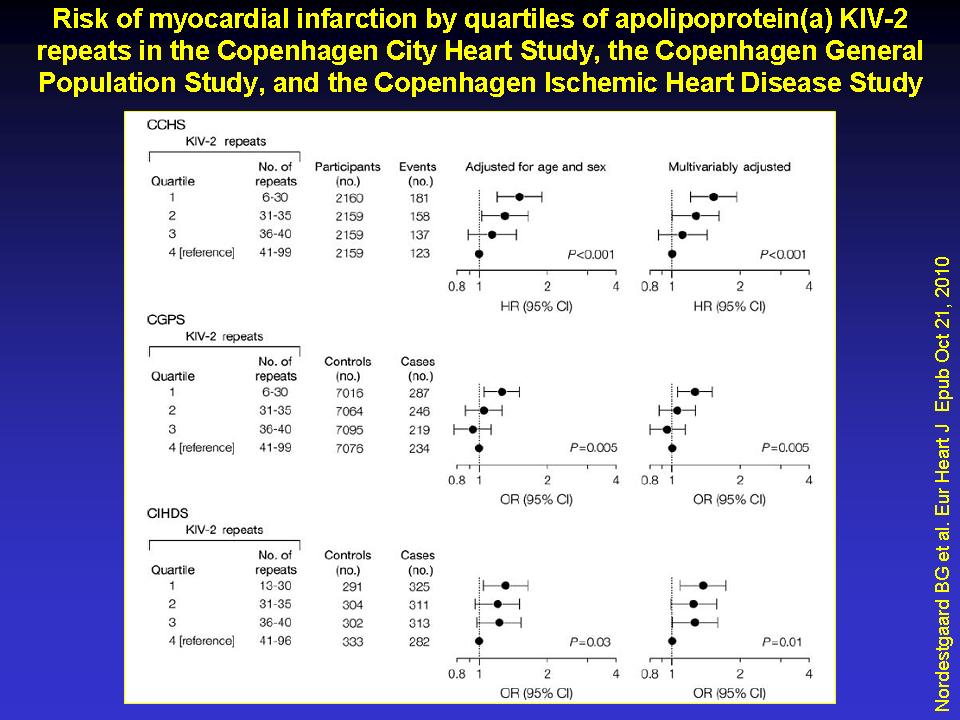
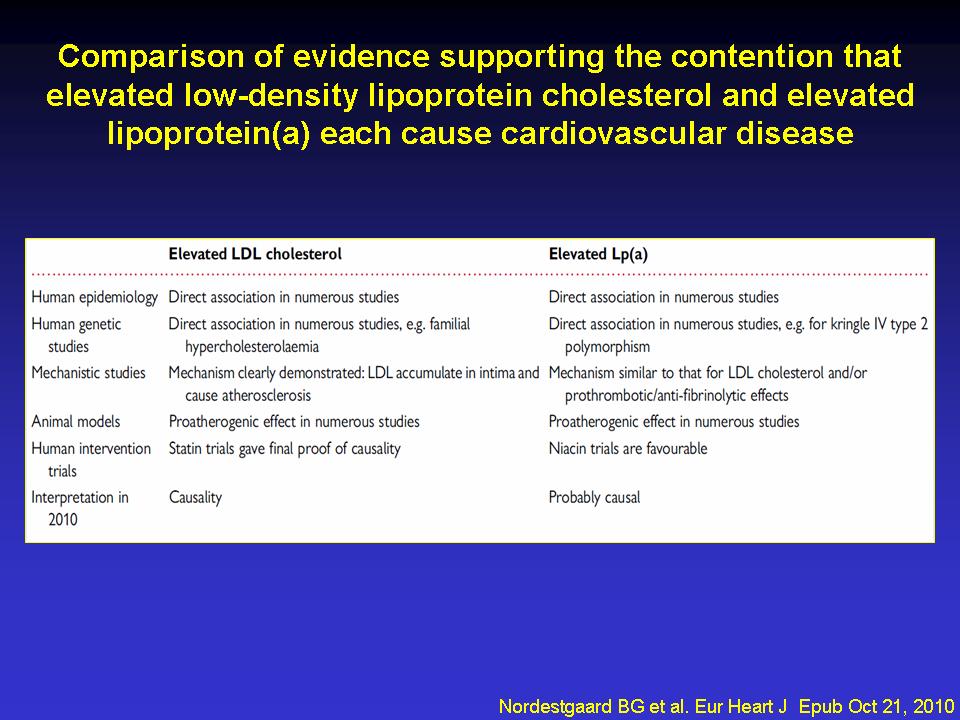
METHODS AND RESULTS: The robust and specific association between
elevated Lp(a) levels and increased cardiovascular disease (CVD)/coronary
heart disease (CHD) risk, together with recent genetic findings,
indicates that elevated Lp(a), like elevated LDL-cholesterol,
is causally related to premature CVD/CHD. The association is continuous
without a threshold or dependence on LDL- or non-HDL-cholesterol
levels. Mechanistically, elevated Lp(a) levels may either induce
a prothrombotic/anti-fibrinolytic effect as apolipoprotein(a)
resembles both plasminogen and plasmin but has no fibrinolytic
activity, or may accelerate atherosclerosis because, like LDL,
the Lp(a) particle is cholesterol-rich, or both. We advise that
Lp(a) be measured once, using an isoform-insensitive assay, in
subjects at intermediate or high CVD/CHD risk with premature CVD,
familial hypercholesterolaemia, a family history of premature
CVD and/or elevated Lp(a), recurrent CVD despite statin treatment,
=3% 10-year risk of fatal CVD according to European guidelines,
and/or =10% 10-year risk of fatal + non-fatal CHD according to
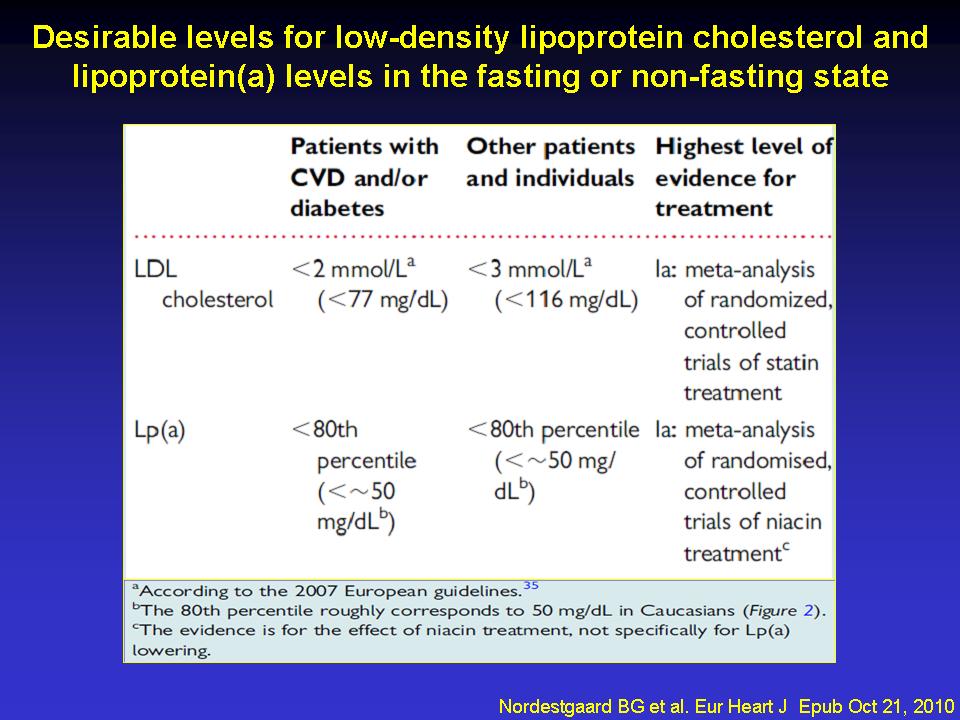
US guidelines. As a secondary priority after LDL-cholesterol reduction,
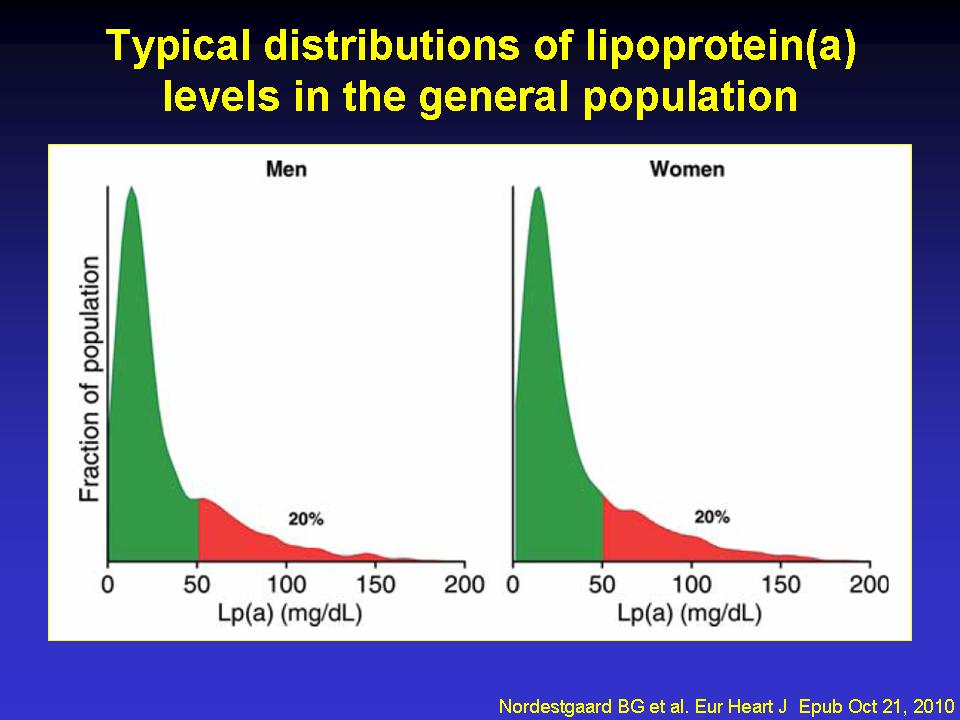
we recommend a desirable level for Lp(a) <80th percentile (less
than ~50 mg/dL). Treatment should primarily be niacin 1-3 g/day,
as a meta-analysis of randomized, controlled intervention trials
demonstrates reduced CVD by niacin treatment. In extreme cases,
LDL-apheresis is efficacious in removing Lp(a).
CONCLUSION: We recommend screening for elevated Lp(a) in those
at intermediate or high CVD/CHD risk, a desirable level <50
mg/dL as a function of global cardiovascular risk, and use of
niacin for Lp(a) and CVD/CHD risk reduction.
|
|