| Abstract
|
OBJECTIVE: To evaluate the incremental cost-effectiveness ratio
(ICER) of switching to ezetimibe/simvastatin (Eze/Simva) compared
with doubling the submaximal statin doses, in patients with acute
coronary syndrome (ACS) events in the INFORCE study.
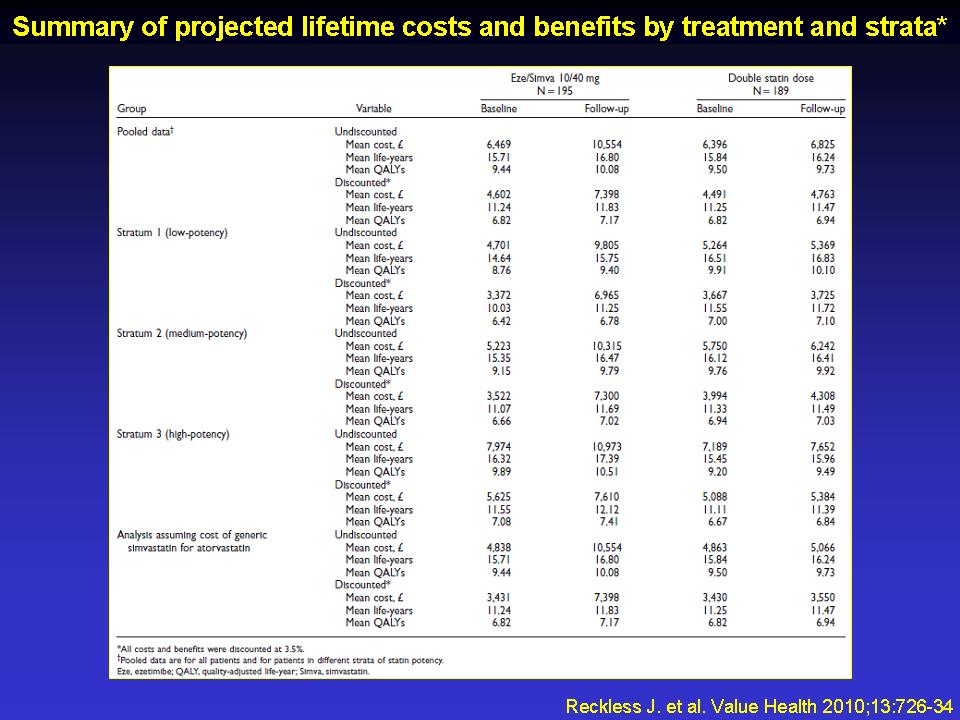
METHODS: Lifetime treatment costs and benefits were computed using
a Markov model. Model inputs included each patient's cardiovascular
risk factor profile and actual lipid values at baseline and 12
weeks (endpoint). Cardiovascular event and drug costs were discounted
at 3.5%. Age-specific utilities were based on UK literature values
and non-coronary heart disease mortality rates on the Office of
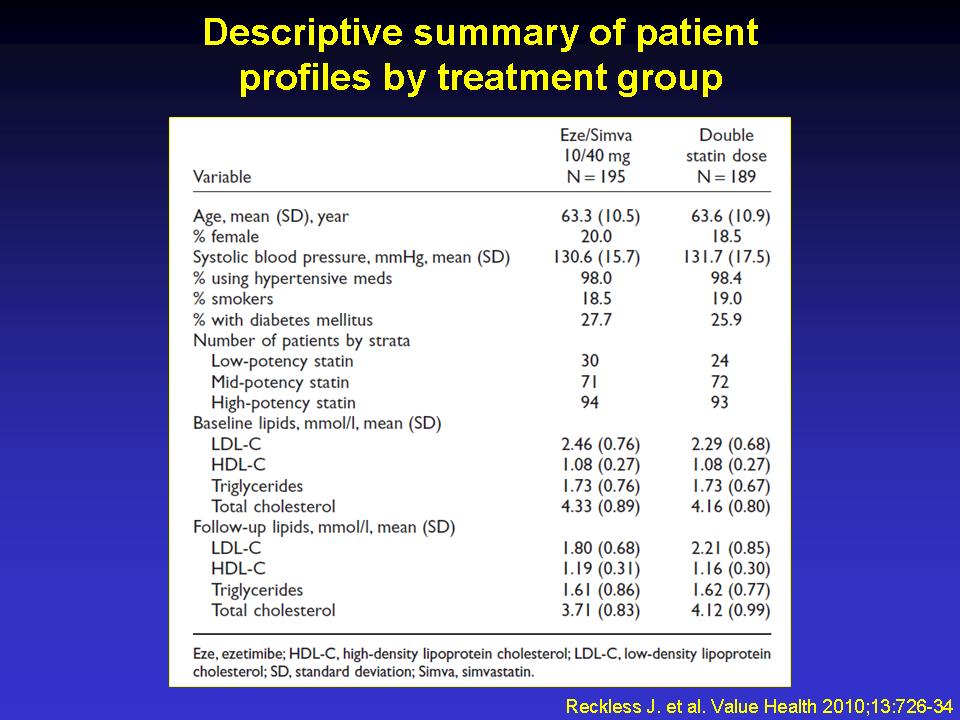
National Statistics data. In the INFORCE study, 384 patients taking
statins at stable doses for =6 weeks before hospital admission
were stratified by statin dose/potency (low, medium, and high)
and then randomized to doubling the statin dose or switching to
Eze/Simva 10/40mg for 12 weeks.
RESULTS: The Eze/Simva group (n=195) had a higher mean baseline
total cholesterol than the double-statin group (n=189). Analyses
were adjusted for baseline characteristics. In the INFORCE study,
Eze/Simva reduced low-density lipoprotein cholesterol (LDL-C)
by ~30% (vs. 4% with doubling statin doses) and significantly
enhanced LDL-C goal attainment. In the cost-effectiveness analysis,
Eze/Simva conferred 0.218 incremental discounted quality-adjusted
life year (QALY) at a discounted incremental cost of £2524,
for an ICER of £11,571/QALY (95% confidence interval=£8181-£18,600/QALY).
The ICER was £13,552/QALY, £11,930/QALY, and £10,148/QALY
in the low-, medium-, and high-potency strata, respectively.
CONCLUSIONS: Switching to Eze/Simva 10/40 mg is projected to be
a cost-effective treatment (vs. double-statin) in UK patients
with ACS.
|