| Authors |
Colin
Baigent, Martin J Landray, Christina Reith, Jonathan Emberson,
David C Wheeler, Charles Tomson, Christoph Wanner, Vera Krane,
Alan Cass, Jonathan Craig, Bruce Neal, Lixin Jiang, Lai Seong
Hooi, Adeera Levin, Lawrence Agodoa, Mike Gaziano, Bertram Kasiske,
Robert Walker, Ziad A Massy, Bo Feldt-Rasmussen, Udom Krairittichai,
Vuddidhej Ophascharoensuk, Bengt Fellström, Hallvard Holdaas,
Vladimir Tesar, Andrzej Wiecek, Diederick Grobbee, Dick de Zeeuw,
Carola Grönhagen-Riska, Tanaji Dasgupta, David Lewis, William
Herrington, Marion Mafham, William Majoni, Karl Wallendszus, Richard
Grimm, Terje Pedersen, Jonathan Tobert, Jane Armitage, Alex Baxter,
Christopher Bray, Yiping Chen, Zhengming Chen, Michael Hill, Carol
Knott, Sarah Parish, David Simpson, Peter Sleight, Alan Young,
Rory Collins
|
| Abstract
|
Background: Lowering LDL cholesterol with statin regimens reduces
the risk of myocardial infarction, ischaemic stroke, and the need
for coronary revascularisation in people without kidney disease,
but its effects in people with moderate-to-severe kidney disease
are uncertain. The SHARP trial aimed to assess the efficacy and
safety of the combination of simvastatin plus ezetimibe in such
patients.
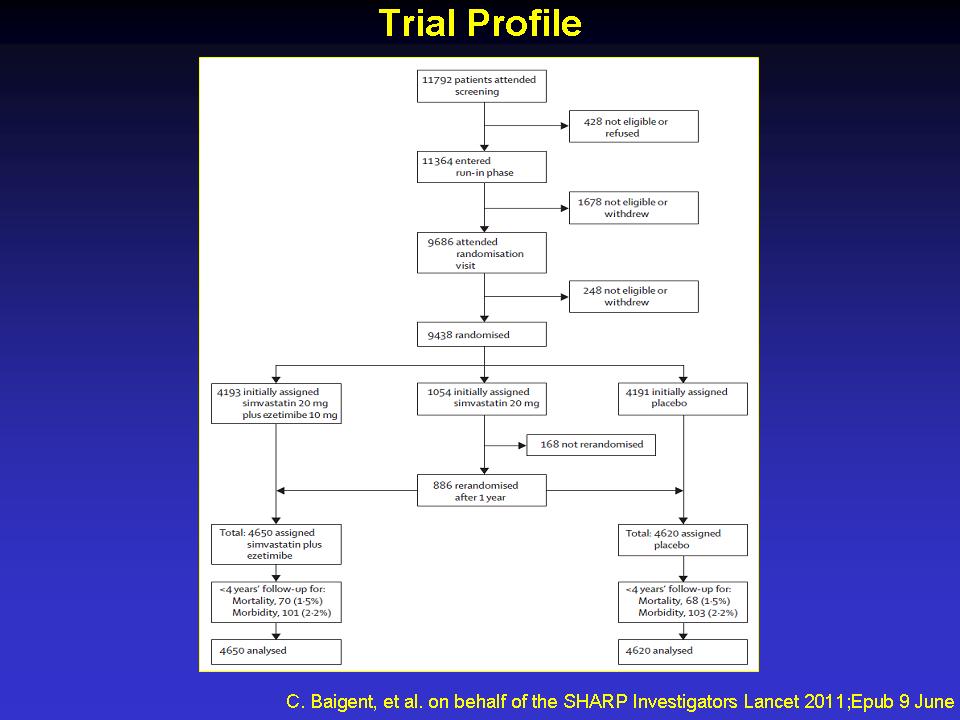
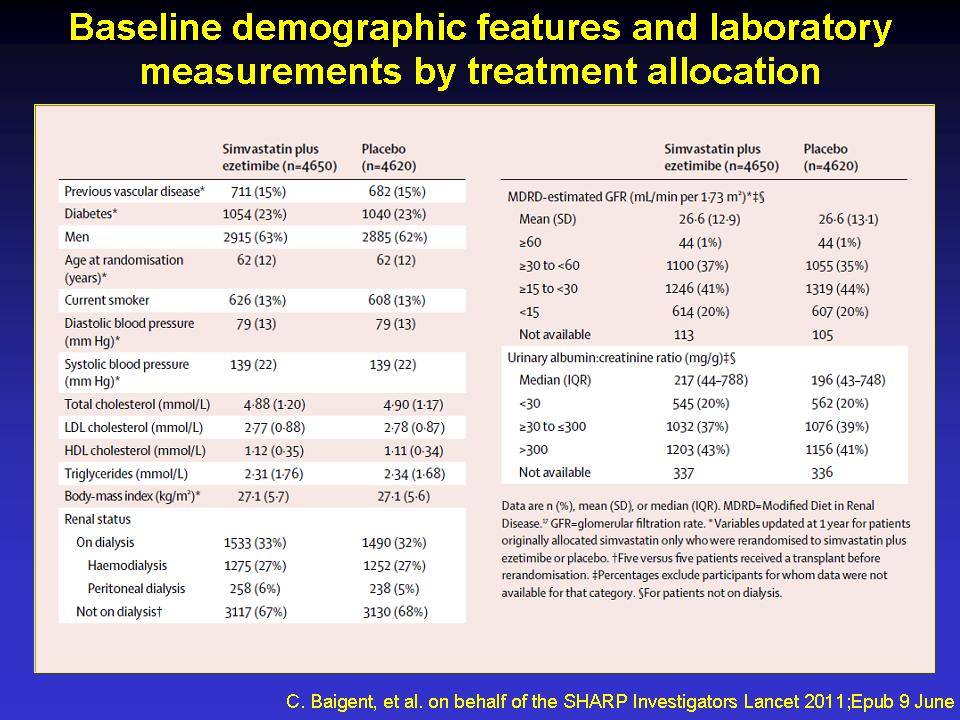
Methods: This randomised double-blind trial included 9270 patients
with chronic kidney disease (3023 on dialysis and 6247 not) with
no known history of myocardial infarction or coronary revascularisation.
Patients were randomly assigned to simvastatin 20 mg plus ezetimibe
10 mg daily versus matching placebo. The key prespecified outcome
was first major atherosclerotic event (non-fatal myocardial infarction
or coronary death, non-haemorrhagic stroke, or any arterial revascularisation
procedure). All analyses were by intention to treat. This trial
is registered at ClinicalTrials.gov, NCT00125593, and ISRCTN54137607.
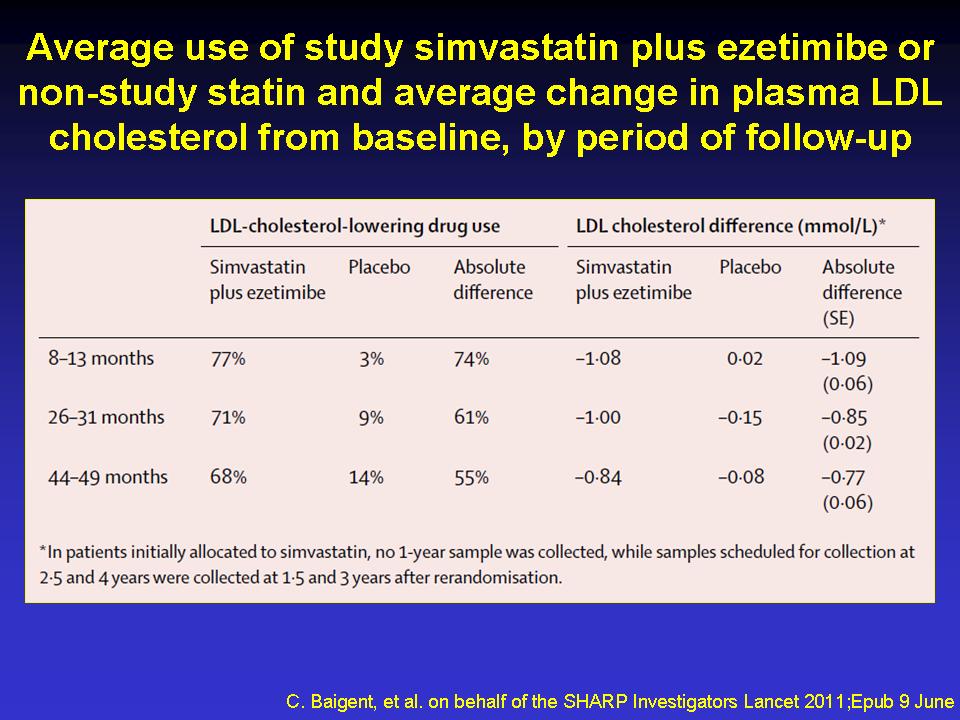
Findings: 4650 patients were assigned to receive simvastatin plus
ezetimibe and 4620 to placebo. Allocation to simvastatin plus
ezetimibe yielded an average LDL cholesterol difference of 0.85
mmol/L (SE 0.02; with about two-thirds compliance) during a median
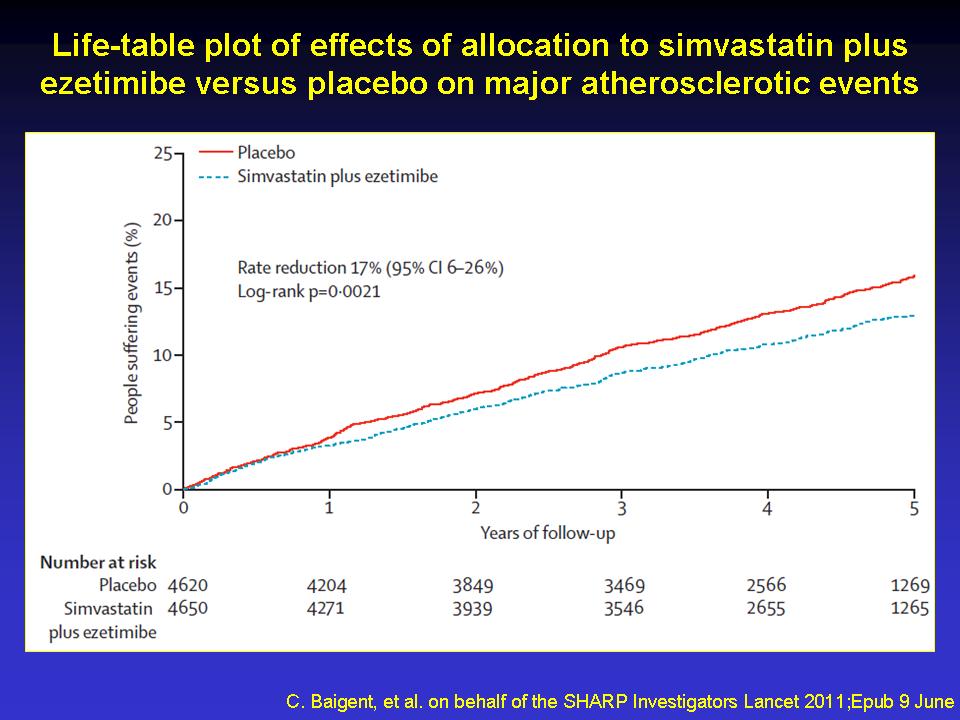
follow-up of 4.9 years and produced a 17% proportional reduction
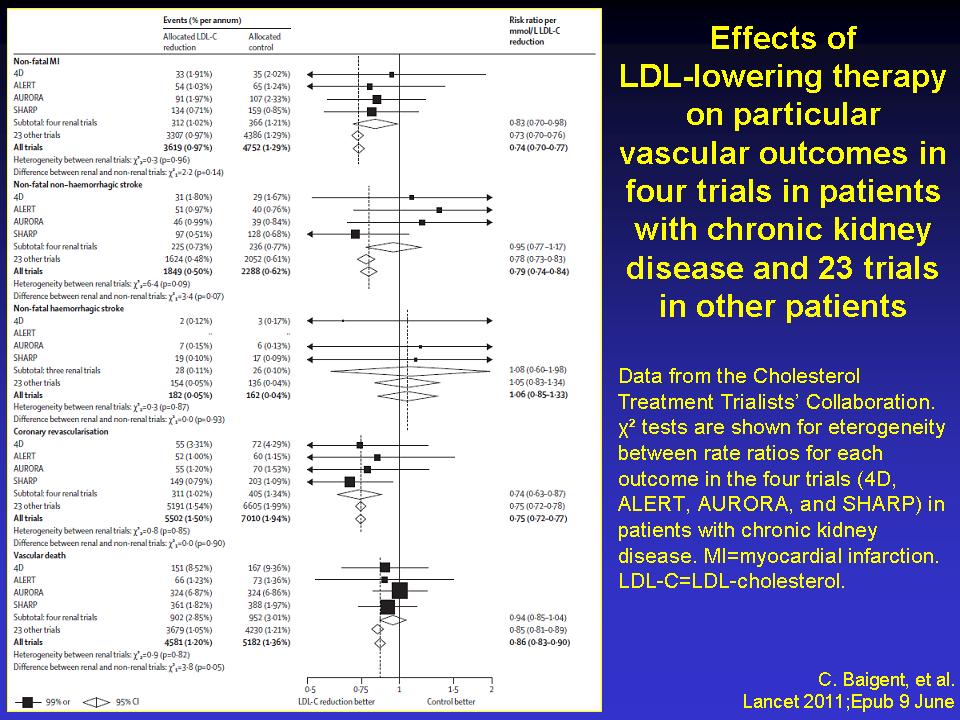
in major atherosclerotic events (526 [11·3%] simvastatin
plus ezetimibe vs 619 [13.4%] placebo; rate ratio [RR] 0.83, 95%
CI 0.74—0.94; log-rank p=0.0021). Non-significantly fewer
patients allocated to simvastatin plus ezetimibe had a non-fatal
myocardial infarction or died from coronary heart disease (213
[4.6%] vs 230 [5.0%]; RR 0.92, 95% CI 0.76—1.11; p=0.37)
and there were significant reductions in non-haemorrhagic stroke
(131 [2.8%] vs 174 [3.8%]; RR 0.75, 95% CI 0.60—0.94; p=0.01)
and arterial revascularisation procedures (284 [6.1%] vs 352 [7.6%];
RR 0.79, 95% CI 0.68—0.93; p=0.0036). After weighting for
subgroup-specific reductions in LDL cholesterol, there was no
good evidence that the proportional effects on major atherosclerotic
events differed from the summary rate ratio in any subgroup examined,
and, in particular, they were similar in patients on dialysis
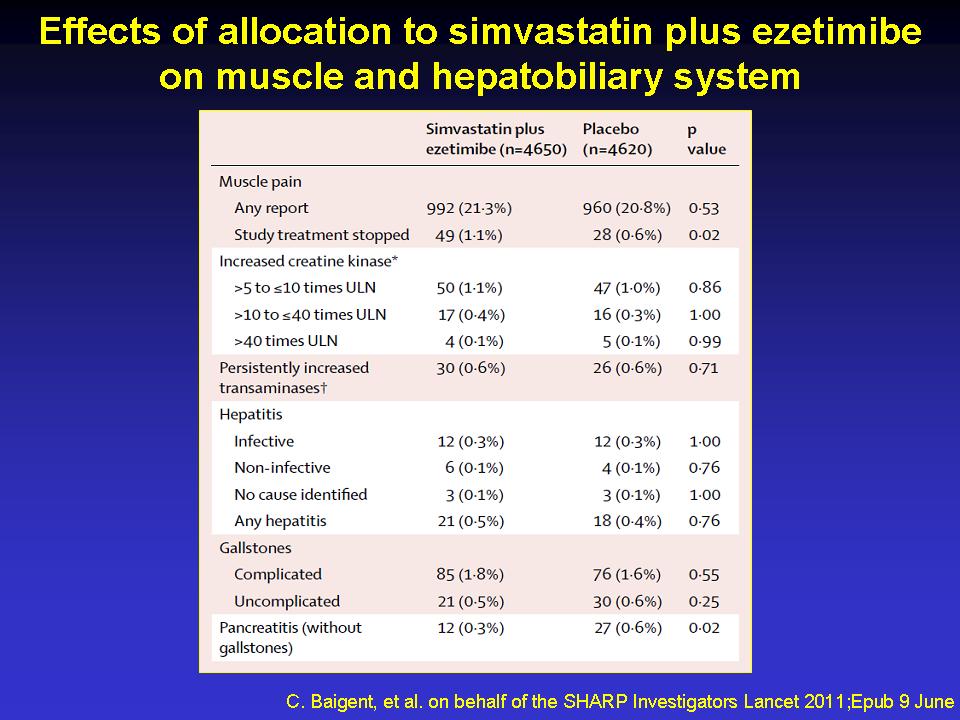
and those who were not. The excess risk of myopathy was only two
per 10 000 patients per year of treatment with this combination
(9 [0.2%] vs 5 [0.1%]). There was no evidence of excess risks
of hepatitis (21 [0.5%] vs 18 [0.4%]), gallstones (106 [2.3%]
vs 106 [2.3%]), or cancer (438 [9.4%] vs 439 [9.5%], p=0·89)
and there was no significant excess of death from any non-vascular
cause (668 [14.4%] vs 612 [13.2%], p=0.13).
Interpretation: Reduction of LDL cholesterol with simvastatin
20 mg plus ezetimibe 10 mg daily safely reduced the incidence
of major atherosclerotic events in a wide range of patients with
advanced chronic kidney disease.
Funding: Merck/Schering-Plough Pharmaceuticals; Australian National
Health and Medical Research Council; British Heart Foundation;
UK Medical Research Council.
|