| Authors |
Heart
Protection Study Collaborative Group, Jonathan Emberson, Derrick
Bennett, Emma Link, Sarah Parish, John Danesh, Jane Armitage,
Rory Collins.
|
| Abstract
|
BACKGROUND: It has been suggested that inflammation status, as
assessed by C-reactive protein (CRP) concentration, modifies the
vascular protective effects of statin therapy. In particular,
there have been claims that statins might be more beneficial in
people with raised CRP concentrations, and might even be ineffective
in people with low concentrations of both CRP and LDL cholesterol.
This study aimed to test this hypothesis.
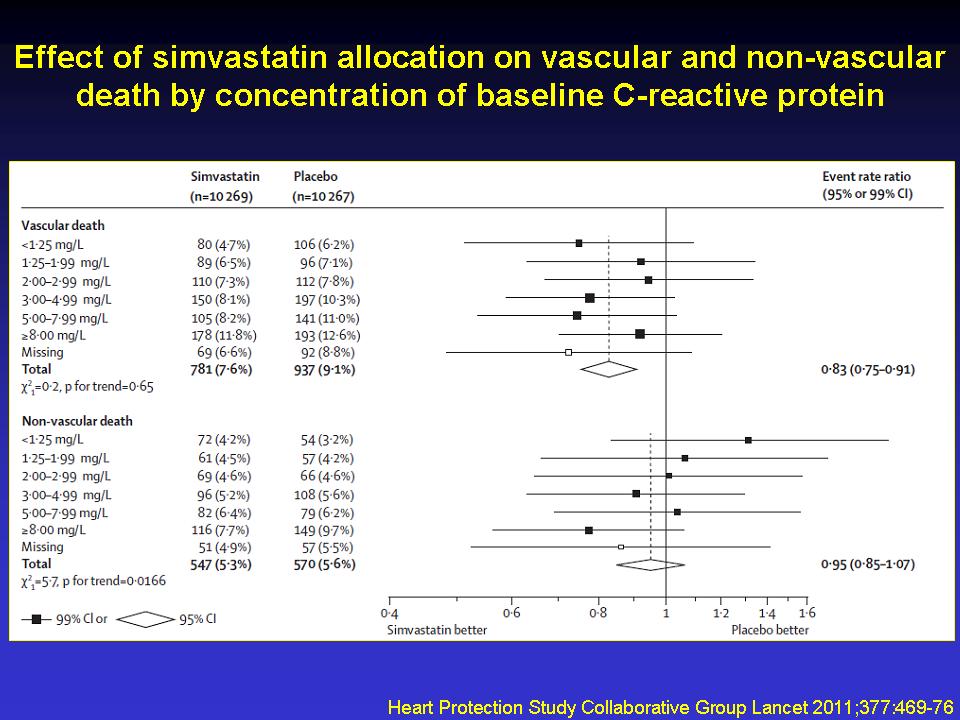
METHODS: In 69 UK hospitals, 20,536 men and women aged 40-80 years
at high risk of vascular events were randomly assigned to simvastatin
40 mg daily versus matching placebo for a mean of 5·0 years.
Patients were categorised into six baseline CRP groups (<1·25,
1·25-1·99, 2·00-2·99, 3·00-4·99,
5·00-7·99, and =8·00 mg/L). The primary endpoint
for subgroup analyses was major vascular events, defined as the
composite of coronary death, myocardial infarction, stroke, or
revascularisation. Analysis was by intention to treat. This study
is registered, number ISRCTN48489393.
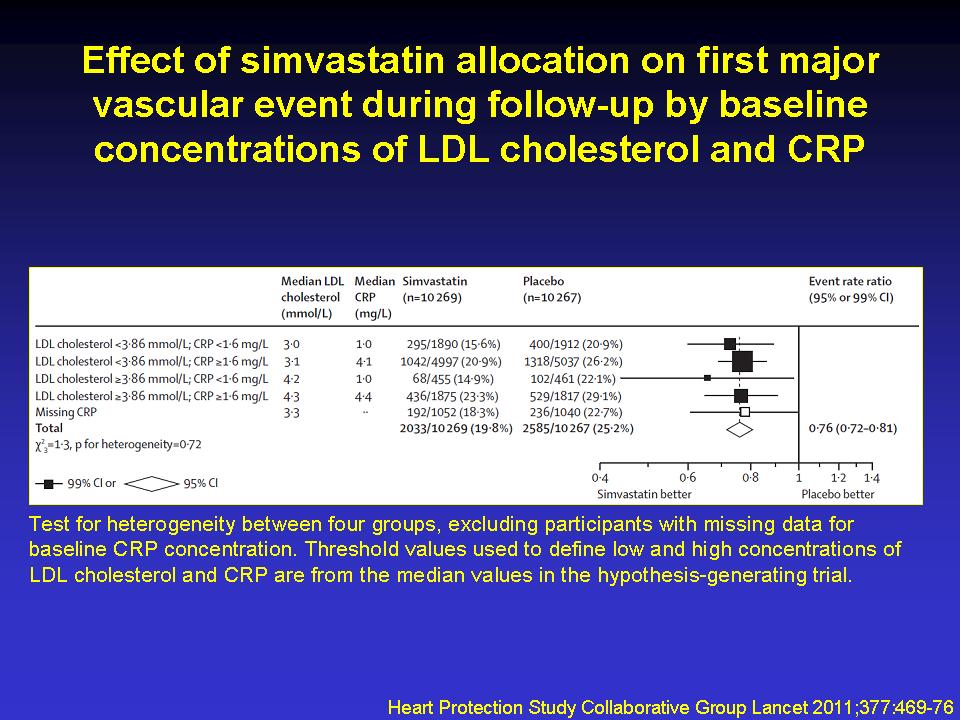
FINDINGS: Overall, allocation to simvastatin resulted in a significant
24% (95% CI 19-28) proportional reduction in the incidence of
first major vascular event after randomisation (2033 [19·8%]
allocated simvastatin vs 2585 [25·2%] allocated placebo).
There was no evidence that the proportional reduction in this
endpoint, or its components, varied with baseline CRP concentration
(trend p=0·41). Even in participants with baseline CRP
concentration less than 1·25 mg/L, major vascular events
were significantly reduced by 29% (99% CI 12-43, p<0·0001;
239 [14·1%] vs 329 [19·4%]). No significant heterogeneity
in the relative risk reduction was recorded between the four subgroups
defined by the combination of low or high baseline concentrations
of LDL cholesterol and CRP (p=0·72). In particular, there
was clear evidence of benefit in those with both low LDL cholesterol
and low CRP (27% reduction, 99% CI 11-40, p<0·0001;
295 [15·6%] vs 400 [20·9%]).
INTERPRETATION: Evidence from this large-scale randomised trial
does not lend support to the hypothesis that baseline CRP concentration
modifies the vascular benefits of statin therapy materially.
FUNDING: UK Medical Research Council, British Heart Foundation,
Merck, Roche Vitamins, and GlaxoSmithKline.
|